Su H, Gonzalez-Martin O, Weisgold A, Lee E Considerations of implant abutment and crown contour: critical contour and subcritical contour. Int J Periodontics Restorative Dent. 2010; 30:335-343
González-Martín O, Lee E, Weisgold A Contour management of implant restorations for optimal emergence profiles: guidelines for immediate and delayed provisional restorations. Int J Periodontics Restorative Dent. 2020; 40:61-70 https://doi.org/10.11607/prd.4422
Top Tips Kyle D Hogg Aesthetic Update 2025 1:3, 163-164.
Authors
Kyle DHogg
DDS, MClinDent Prosthodontics, FICD, FCGDent, Principal, Dental Health Professionals Private Practice, Cadillac, MI, USA; Editorial Board Member and Faculty, Academy of Dental Excellence; Clinical Teacher and Postgraduate Tutor, MSc Aesthetic Dentistry Programme, King's College London Faculty of Dentistry, Oral and Craniofacial Sciences, London
Controlling white and pink aesthetics is important in predictably providing patients with aesthetic implant restorations. Understanding how the contours of the abutment and crown can be prescribed, manipulated, and confirmed can hold the key to success.
Article
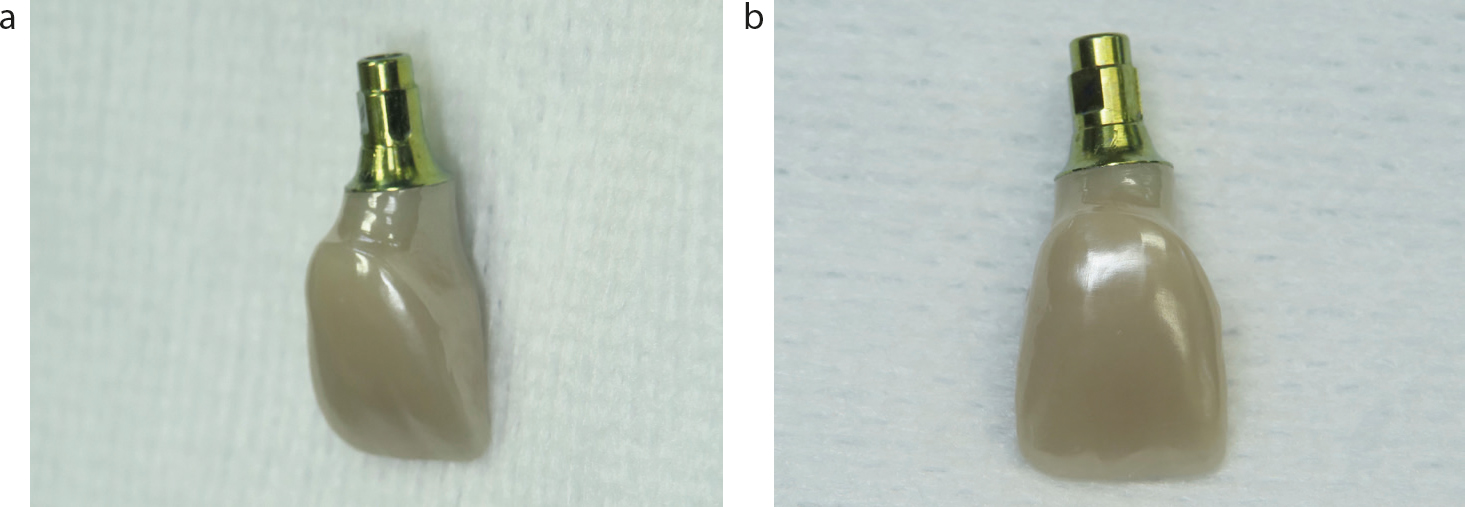
An ideally contoured implant abutment/crown complex needs to transition from the implant platform and emerge through the peri-implant tissues, providing the correct cervical tooth anatomy (Figure 1). Generally speaking, implant restorations have been described as overcontoured, flat or undercontoured. Overcontouring of the emergence profile tends to exert pressure upon the tissues and can result in a more apical migration of the gingival margin, while undercontouring will alleviate pressure and encourage a more coronal migration of the gingival margin.1 Knowing how and where to adjust restorative contours can be the difference between an aesthetic or deficient outcome.
Figure 1.
(a,b) A contoured implant abutment/crown complex.
It is important to define the transmucosal portion of the abutment/crown complex into two distinct zones: the critical contour (the area shaded blue in Figure 2) and the subcritical contour (the area shaded pink in Figure 2).2 The design of the critical contour should correlate to the desired gingival anatomy that is being created. The facial profile of the critical contour is particularly important in determining the height and location of the gingival zenith. The deeperlying subcritical contour influences the peri-implant soft-tissue support and thickness and, consequently, gingival colour and profile.3
Figure 2. The transmucosal portion of the abutment/crown complex can be defined into two distinct zones: the critical contour (shaded blue) and the subcritical contour (shaded pink).
When seating an implant restoration, such as the screw-retained monolithic 4Y zirconia provisional crown on a gold-anodized Ti-base abutment seen in Figure 3, pay particular attention to any blanching of the peri-implant gingival tissues that lasts for more than 5 minutes. Residual blanching may reveal excessive pressure from an inappropriate contour. Avoiding administration of anaesthetic, particularly those that contain a vasoconstrictor, is important to allow for proper assessment. Step away from the surgery, check a hygiene patient, answer an email, or grab a quick espresso – just allow the tissue to settle! If the gingival colour returns to normal colouration, then the blood supply has been re-established. If blanching is persistent consider alteration of the subcritical contour to alleviate pressure and repeat the observation period.
Figure 3. Blanching of the peri-implant gingival tissues following seating an implant restoration.
Once the peri-implant tissue colour and subcritical contours are deemed satisfactory, closely evaluate the critical contour and position of the gingival marginal tissues (Figure 4). Alterations to the vertical position of the marginal tissues and zenith location can be achieved by correcting the position of the critical contour.
Figure 4. Peri-implant tissue colour and subcritical contours were deemed satisfactory.
Knowing when, where, why and how to alter the critical and subcritical contours of your implant restorations can help make your clinical practice more rewarding and predictable while reducing stress and chair time.