Hasan HS, Al Azzawi AM, Kolemen A Pattern of distribution and etiologies of midline diastema among Kurdistan-region population. J Clin Exp Dent. 2020; 12:e938-e943 https://doi.org/10.4317/jced.57122
Steigman S, Weissberg Y Spaced dentition. An epidemiologic study. Angle Orthod. 1985; 55:167-176
Sabri N, Ridzwan SBB, Soo SY Smile attractiveness and treatment needs of maxillary midline diastema with various widths: perception among laypersons, dental students, and dentists in Malaysia. Int J Dent. 2023; 2023 https://doi.org/10.1155/2023/9977868
Flores-Mir C, Silva E, Barriga MI Lay person's perception of smile aesthetics in dental and facial views. J Orthod. 2004; 31:204-209 https://doi.org/10.1179/146531204225022416
Silva BP, Jimenez-Castellanos E, Martinez-de-Fuentes R Perception of maxillary dental midline shift in asymmetric faces. Int J Esthet Dent. 2015; 10:588-596
Rogé M, Fisselier F-M A new, more personal vision of esthetics. J Cosmet Dent Winter. 2017; 32:88-105
Van Der Geld P, Oosterveld P, Berge SJ, Kuijpers-Jagtman AM Tooth display and lip position during spontaneous and posed smiling in adults. Acta Odontol Scand. 2008; 66:207-213 https://doi.org/10.1080/00016350802060617
Coachman C, Calamita MA, Sesma N Dynamic documentation of the smile and the 2D/3D digital smile design process. Int J Periodontics Restorative Dent. 2017; 37:183-193 https://doi.org/10.11607/prd.2911
Bapelle M, Dubromez J, Savoldelli C Modjaw device: analysis of mandibular kinematics recorded for a group of asymptomatic subjects. Cranio. 2021; 1-7 https://doi.org/10.1080/08869634.2021.2000790
To bond or not to bond: considerations for choosing the appropriate treatment for closing a midline diastema Elaine Halley Aesthetic Update 2025 1:2, 82-88.
In the realm of dental aesthetics, the decision between employing a resin composite material bonded to the dental hard tissues, or orthodontics to address a midline diastema and enhance smile aesthetics, can be complex and multifaceted. This article delves into the critical considerations and decision-making processes guiding dental practitioners through how to decide when orthodontic movement, while a more costly and complex treatment option, might provide optimum aesthetics. By exploring the aetiology of midline diastemas, and the pivotal role of the central incisor in smile aesthetics the author aims to equip clinicians with a comprehensive framework.
CPD/Clinical Relevance: This article shows how to assess suitable treatment modalities for closing midline diastemas in adult patients.
Article
The presence of a midline diastema in the maxilla, a space between the maxillary central incisors, is a common dental anomaly that can arise for various reasons. This condition, while sometimes considered a characteristic or personality trait, can also be a significant aesthetic concern for many individuals.
The prevalence of maxillary midline diastema varies across different populations and age groups. In the UK, the prevalence has been reported as 3.4%, and globally it has been reported in different populations ranging from 1.6% in certain populations to over 50% in younger age groups and certain ethnic groups.1,2
The decision to close a diastema is largely influenced by the patient's perception of beauty and cultural trends. Famous personalities, such as Madonna, Eddie Murphy, and model, Lara Stone, have been celebrated for their distinctive smiles, which feature a midline diastema. Their visibility has played a role in shifting perceptions, illustrating that beauty is diverse and that a diastema can indeed contribute to a person's charisma and identity.3 While aesthetic concerns are the primary motivation, closing a diastema can also have functional benefits, such as improving occlusion and preventing abnormal tooth wear. Additionally, addressing the diastema may help in managing underlying pathological conditions, such as abnormal frenum attachments or periodontal issues, thereby preventing further dental complications.4
However, patients may present with a request to close the space, and in today's world of social media examples and the ability to research online, patients may also ask for a particular treatment that they have self diagnosed will solve their issue. Unfortunately, although the diagnosis of a midline diastema is straightforward, often the treatment that will provide the best outcome is not obvious. It is important to listen to the patient, but also to diagnose the underlying cause for the space and to undergo a systematic review of the criteria that will provide the optimal aesthetic outcome before undertaking treatment.
Whether the decision is to accept the diastema or to opt for closure through orthodontic or additive procedures, it is essential that treatment plans are patient centred, taking into account the aesthetic desires and psychological wellbeing of the individual.
This article describes the various factors that should be considered when deciding between treatment options, and how to capture the relevant information to allow for treatment planning and patient education.
Aetiology of midline diastemas
Understanding the aetiology of a midline diastema is crucial for clinicians in advising patients on treatment options.5 The aetiology of a midline diastema encompasses a range of factors, including genetic predisposition, developmental anomalies, such as peg lateral incisors in the maxilla, abnormal frenal attachment, and habits such as thumb sucking.6 Genetic predisposition may dictate jaw size and tooth dimension, leading to spacing when teeth are too small relative to the available alveolar bone. Developmental factors, such as the presence of a thick or high labial frenum can also contribute to diastema formation, as can certain habits, for example prolonged thumb sucking, which may exert pressure on teeth and cause separation.
Clinical treatment options for closing a midline diastema
Restoration can be used to change the shape of the tooth with either direct composite material bonded to the dental hard tissues or indirect restorations;
Orthodontic movement of teeth with or without surgical frenectomy.
Options for closing midline diastemas range from restoring teeth to moving teeth,5 and the decision may be influenced by the patient who may state a preference and ask for ‘bonding’, which is a non-dental term associated with the application of direct composite resin, or the patient may ask for orthodontics. However, consideration of both the aetiology of the space and the current clinical situation is essential to determine the correct treatment option and the advantages and disadvantages of different options. When a patient has a diastema in the upper anterior dentition, it is important to consider various factors before deciding on the appropriate treatment option for the patient.
Factors to consider when deciding whether restoration is suitable to close a midline diastema7
The proportion of the central incisors;
The position of the centre of the diastema in relation to the facial midline;
The long axial inclination of the central incisors.
The proportion of the central incisors
The central incisor plays a pivotal role in defining smile aesthetics, acting as a cornerstone for facial harmony and symmetry. As one of the most visible elements in smile dynamics, the shape, size, position and colour of the central incisors significantly influence the perception of a pleasing smile.8 The characteristics and initial proportions of the central incisor can be instrumental in deciding whether this is a case that is suitable for restoration with direct composite material bonded to the dental hard tissues.
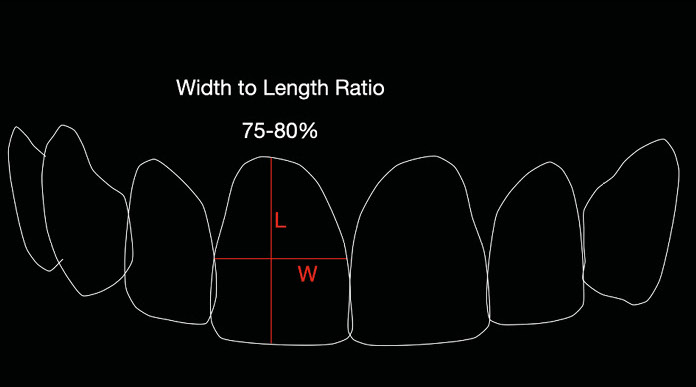
For ideal aesthetics, central incisors should have a 75–80% width-to-length ratio. This means that if a central incisor is 10 mm long, it should be 8 mm in width (Figure 1).
Figure 1. Width to length ratio of a central incisor.
If composite resin is added to the mesial of centrals, this will change the width, which will therefore affect the width:length proportion. For this reason, if the teeth are narrow and the diastema is relatively small (1–2 mm) (Figure 2) then adding some curvature and a contact area can be aesthetically pleasing and keep the ideal proportions (Figure 3). If, on the other hand the teeth are square initially, then adding width can result in the teeth becoming wider than they are tall, which may result in an unaesthetic visual appearance (Figure 4).
Figure 2. This pre-treatment picture illustrates a small diastema and narrow teeth, which would be suitable for composite resin addition to the mesial surfaces.Figure 3. In this post-treatment picture, the diastema has been closed using indirect porcelain restorations on the upper four anteriors to redistribute width-to-length ratios.Figure 4. In this case, the central incisors have a square shape and the addition of composite resin to the mesial surfaces would create an unaesthetic result.
However, this could be overcome by adding to the length to maintain the ratio. To consider this, the incisal edge position should be evaluated according to the face, occlusion and phonetics.9 Is it possible to lengthen the incisors without causing an occlusal interference or a lip trap during speech? Is it possible to lengthen in a gingival direction with crown lengthening, either soft tissue alone, or bone and soft tissue, respecting the biological width? Is the cemento-enamel junction of the incisors visible, or could there have been any altered passive eruption? Has there been any dento-alveolar compensation with wear of the incisal edges?10 In addition, considering crown lengthening for aesthetic purposes may only be relevant in a patient with a high smile. If the patient does not elevate the upper lip sufficiently to show the cervical margin of the central then submitting the patient to a procedure that may include surgery, is not in the best interest of the patient or, indeed, the final aesthetic result.
This issue can also be overcome by treating more than the central incisors. For example, if porcelain veneers are the treatment of choice, treating all the incisors can allow for space distribution to close the space while maintaining aesthetically pleasing proportions.11 This is a more invasive treatment and should be considered carefully, and the preparations guided with a diagnostic wax-up to ensure adequate, but minimal tooth preparation (Figure 4).
The position of the centre of the diastema in relation to the facial midline
One of the first determinants of whether bonding or addition to a tooth will be aesthetically successful is to determine whether the current midline is in the centre of the face. With a good photograph taken in a natural head position, it is possible to use presentation software, such as Keynote (Apple, USA) or PowerPoint (Microsoft, USA), to level the horizontal plane by rotating the picture so that the eyes are level with the horizon. A perpendicular line can be positioned through the centre of the glabella, nose, philtrum and tip of the chin. It is then possible to determine where the diastema lies in relation to the midline.
When considering whether a space should be closed with the application of direct composite resin, visualising what would happen to the position of the midline itself in relation to the face if equal amounts of resin were added to the mesial of each maxillary central incisor might be helpful. If the middle of the diastema is in the middle of the face, then the addition of equal amounts of resin to either side of the diastema should be aesthetically pleasing. If the visual dental midline will be shifted significantly by this approach because the middle of the diastema deviates from the midline of the face, then this may be considered a deviation away from the ideal aesthetic. Central incisors should be symmetrical and so it is not desirable to add uneven amounts of composite resin to central incisors if their width is the same in the first instance. Smile design literature traditionally quotes that a 4-mm deviation from the facial midline can be tolerated as long as the midline is perpendicular to the horizon.12 Recent studies, however, have shown that a 1-mm deviation can be detected by the lay person, and if there is deviation in the face these perceptions can be altered further.13
The long axial inclination of the central incisors
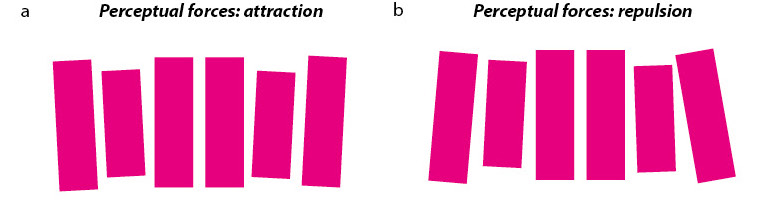
The long axis of an anterior tooth is determined by the line that connects the zenith or height of contour of the gingival curve and the mid-point of the incisal edge. Smile design literature tells us that the central incisors should have a vertical and parallel long axis, and the lateral incisors and canines should have a slight tilt towards the midline. This produces visual harmony and a feeling of attraction.14 If the long axis of any tooth deviates away from the midline, this produces visual tension, for which it is difficult to compensate with additive techniques alone (Figure 5).
Figure 5. Diagrams to illustrate the perceived forces of objects around the midline. (a) Attraction; (b) repulsion.
Other factors that may influence decision making
In some cases, the aesthetic outcome will not easily be achieved with composite bonding alone. In others, orthodontics may not be appropriate, particularly if the space is small. In some cases, the pros and cons of either treatment can be considered and discussed with the patient (Table 1).
Table 1.
Advantages and disadvantages of diastema closure through orthodontics versus direct composite bonding.
Aspect
Orthodontics
Composite bonding
Treatment duration
May take several months to a year
Can be completed in a single visit
Aesthetic outcome
Natural looking
Immediate results, but may require periodic maintenance. There may be shade match challenges
Preservation of tooth structure
Minimal alteration of tooth structure
Requires alteration of tooth enamel with bonding resin
Longevity
Stable results if retention protocol is followed
May require periodic replacement and be prone to chipping, particularly in bruxists
Adjacent tooth involvement
May involve adjacent tooth movement
No involvement of adjacent teeth
Cost
Higher initial investment
Lower initial cost, but may add up over time with maintenance
Clinical workflow to aid decision making
When evaluating a case to decide which is the appropriate treatment, it is an effective strategy to gather clinical information initially, so that the patient may leave and the clinician can study the various options.
With a digital workflow, it is possible to create a digital avatar of the patient so that many of the critical decisions can be made without the need to decide instantly, or the pressure of giving the patient the correct information in an initial appointment. Time away from the patient can be allocated to analyse the case, and the patient can be invited back for a second consultation to present findings and discuss possible treatment outcomes. This allows the patient, and the practitioner, to consider the risks and benefits of all the treatment options and to come to a decision that has been made with understanding and valid consent.
The information gathered should include:
Full-face photographs taken from the front. Ideally not in the dental chair, but in an upright position with the teeth slightly apart. If there is a true low smile line, this can be evaluated during speech and laughter, and ideally, with a short video clip that allows the clinician to see how much tooth display occurs in dynamic, spontaneous expression compared with posed or static smiling. Studies have shown that there can be 30% more height of display in the premolar region during spontaneous smiling compared with posed smiling;15,16
Digital scan or study model impressions;
Occlusal bite record static and dynamic, digital or analogue. Video of simulated chewing or tracking, for example with a digital bite recorder, such as Modjaw (Modjaw Inc, France) or notes obtained from direct visualisation can dictate the pathway of the mandibular anterior teeth in relation to the diastemas;17
Facial measurements, such as mid-face:lower face, lip length, the length of the central incisor10 will allow for assessment of facial limitations;
Full clinical assessment, including necessary radiographs and periodontal charts.
Simulating possible outcomes
The decision may also be aided by simulating the possible outcome to evaluate how it may look and allow the patient and the clinician to make an informed decision before committing to treatment.
Tools for simulating the possible outcome include:
Direct addition of flowable or regular composite without adhesion can simulate the end result and allow the dentist and the patient to visualise the proposed changes to the dentition;
Trial smile: having an analogue or a digital wax-up with a silicone stent, and using a bisacryl resin-based composite material can simulate additive techniques, and photographs and/or video can be taken to show the effect from different angles.11 This wax-up can be carried out by a dental technician or by using tooth libraries in a software design program;
Orthodontic simulation: software programmes can demonstrate how the teeth may move and also place restorations, and include the changes in a patient's wide-smile, full-face picture.
Other smile simulation software can simulate altering the smile to allow the effects to be viewed as a motivational image;
Apps can provide a very quick alignment of teeth. However, there is no control from the clinician and sometimes the outcomes can vary.
Case study
A 19-year-old patient attended for an opinion about the addition of composite resin as an option to close her midline diastema. Although the patient had other spaces in the anterior dentition, her main concern was the space between her central incisors. Previously, composite resin had been added to the mesial of both upper central incisors, but she had disliked the result and had insisted that the dentist remove the restorative material. She was now seeking a superior aesthetic outcome, which she believed could still be achieved by the addition of composite resin material (Figure 6).
Figure 6. Pre-treatment frontal view in retraction.
At the initial examination, an intra-oral scan and clinical photographs were taken. A systematic aesthetic review showed:
The current width:length ratio would be distorted by adding composite to the mesial of the centrals, possibly why the initial result had been displeasing;
The lip at full mobility did not reveal the gingival margin of the maxillary central incisors and so crown lengthening would not be appropriate to overcome this;
The patient had a microdontic lateral incisor that was contributing to the excess space;
The patient had a small maxilla compared to her mandible, and the maxilla was retrognathic in profile. She had reduced mid-face length compared to her lower face. This means that there was a structural reason for her lack of tooth display. Orthognathic surgery as an option was discussed, but declined;
The long axes of the central incisors deviated away from the midline, which was an indication that modifying their shape with the addition of composite resin to obtain the correct angulation could be challenging. This was in part due to the position of the curve of the gingival margin, which could not be disguised by restoration alone;
The position of the incisal edge of the maxillary central incisors was at an appropriate position in her smile and did not require to be lengthened incisally;
There was a low upper frenal attachment.
All the above factors were discussed with the patient, using photographs and the intra-oral scan to aid communication. Once she understood why the addition of composite resin alone would not solve the aesthetic issues, she decided to proceed with orthodontic alignment to close the space between the upper central incisors. Space was left around the microdontic upper right lateral incisor so that it could be restored with composite resin or porcelain at a later date (Figures 7 and 8). The patient was delighted with the final result and understood the requirement for retention.
Figure 7. Post-orthodontic treatment with clear aligners. The bur marks are a result of attachment removal and pre-polishing.Figure 8. Final result.
The financial and time investment in orthodontics compared with composite bonding are significant. By performing a thorough analysis, listening to the patient and also considering alternative options with the use of visual aids to explain the options, helped the patient to come to this decision.
Conclusion
Closing a midline diastema in an adult patient involves careful consideration of aesthetic desires, functional implications, and the underlying causes. The position and the initial proportions of the central incisor can dictate whether simple bonding is possible, or whether a more comprehensive approach is required with orthodontics. The decision should align with the patient's vision and wellbeing, supported by professional guidance to achieve the best outcome.