Albwardi M, Albwardi S, Dobaian K The influence of maxillary incisor labiolingual inclination on smiling profile esthetics among Saudis. Cureus. 2022; 14 https://doi.org/10.7759/cureus.20966
Cochrane SM, Cunningham SJ, Hunt NP A comparison of the perception of facial profile by the general public and 3 groups of clinicians. Int J Adult Orthodon Orthognath Surg. 1999; 14:291-295
Swift A, Liew S, Weinkle S The facial aging process from the ‘inside out’. Aesthet Surg J. 2021; 41:1107-1119 https://doi.org/10.1093/asj/sjaa339
Bae GY, Na JI, Park KC, Cho SB Nonsurgical correction of drooping mouth corners using monophasic hyaluronic acid and incobotulinumtoxin A. J Cosmet Dermatol. 2020; 19:338-345 https://doi.org/10.1111/jocd.13010
Coimbra DD, Stefanello B Myomodulation with facial fillers: a comprehensive technical guide and retrospective case series. Aesthetic Plast Surg. 2023; 47:1162-1174 https://doi.org/10.1007/s00266-022-03193-y
Fatani B An approach for gummy smile treatment using botulinum toxin A: a narrative review of the literature. Cureus. 2023; 15 https://doi.org/10.7759/cureus.34032
The aesthetics industry is still unregulated in the UK, and with the surge in people seeking facial aesthetic procedures, there has been a concomitant increase in the incidence of complications associated with these procedures. Dentists are especially well positioned to undertake facial aesthetic treatments providing that they have the appropriate training. Dentists generally have a strong foundational understanding of facial anatomy, in particular skeletal jaw structure, musculature, nerve and main vascular supply. In particular, dentists are exceptionally insightful around the peri-oral region and the smile.
CPD/Clinical Relevance: There are many parallels and transferable skills between dentistry and facial aesthetics and dentists are well positioned to undertake facial aesthetic treatments after appropriate training.
Article
Over the past 10 years, there has been a surge in dentists training in facial aesthetics and adding this into their treatment armamentarium. With the unfortunate reality that the aesthetics industry is still unregulated in the UK, and the resultant growing incidence of aesthetic complications, patients are seeking highly skilled dental and medical professionals. Dentists are especially well positioned to undertake facial aesthetic treatments with the appropriate focused training. This is particularly true because of the many parallels and transferable skills between dentistry and facial aesthetics.
Dentists generally have a strong foundational understanding of facial anatomy, in particular the skeletal jaw structure, musculature, nerve and main vascular supply. In particular, dentists are exceptionally insightful around the peri-oral region and the smile, which are heavy contributors to the overall aesthetic of a face. Indeed, it is within the remit of a dentist to correctly diagnose a skeletal malocclusion (chin position relative to maxilla) or to understand the impact of musculoskeletal discrepancies on lip function and aesthetics. Dentists are therefore in a position to assess the face in great depth, particularly when this knowledge is coupled with manual dexterity, an aesthetic eye and an aptitude for precision.
Some of the applications of dentistry in facial aesthetics include, but are not limited to, the disguising of skeletal Class 2 and 3 malocclusions through lip, chin, and mid-face augmentations, treatment of bruxism-related masseter hypertrophy, management of gummy smiles caused by hyperactivity of the levator labii superioris alequi nasi muscles, hyperactive mentalis or depressor anguli oris muscles, and the treatment of ptotic oral commissures as a result of a reduced occlusal vertical dimension due either to tooth loss or the impacts of ageing.
While the natural process of ageing involves resorption of all aspects of the mandible. The shortening of the chin height and lower facial third, can be easily appreciated from frontal assessments of facial changes during the ageing process (Figure 1). Tooth loss, can be a contributing factor to irreversible alveolar bone resorption, as is well understood by dentists, further exacerbating the extent of reduction in the dimension of the lower facial third and the appearance of mandibular retrognathia.1
Figure 1. The changes that occur during ageing.
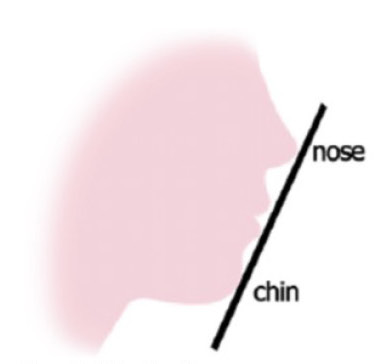
Additionally, the influence of proclined incisors, or bi-maxillary proclination. Is another example of the influence of tooth position on facial profile (Figure 2).2
Figure 2. A Class 1 profile.
Indeed, therefore, there is a clear interface between dentistry and facial aesthetics.
A few studies aimed at evaluating perceived attractiveness of Class 1 versus Class 2 or Class 3 facial profiles have been attempted, evaluating the perception of the general public, clinicians, and the individual subjects. Class 1 profiles were perceived to be the most attractive by most groups.3,4 As such, the aim of achieving a Class 1 appearance in facial profile has long been established in both orthodontics and orthognathic surgery. It is therefore highly sought after as a non-surgical treatment, aimed at creating the perception of a Class 1 profile where possible.
Impact of facial aesthetics on smile design
Aesthetic treatments around the perio-oral region can complement smile design and, therefore, can be integrated into smile makeover treatment plans.
The lips frame the smile, and overall harmony between the lips and the teeth can be enhanced by neuromodulation with neurotoxin, or muscle modulation with soft tissue filler augmentation by influencing lip position, lip inversion/eversion, and projection. By the same token, jaw position and tooth position can affect lip aesthetics, contributing to lip asymmetry, increased lip aversion, or lip catching.
Facial ageing
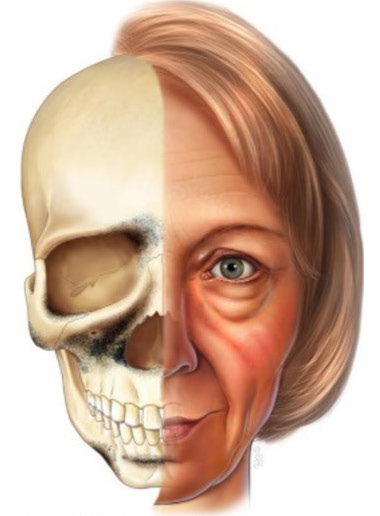
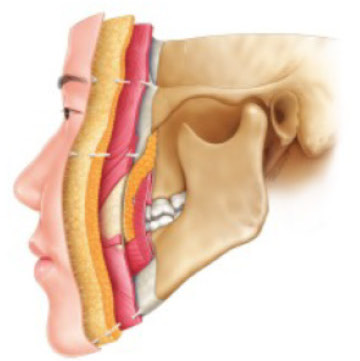
It is worth noting that the perio-oral tissues may undergo several changes with age (Figure 3). The facial ageing process involves changes within every facial layer, of which there are normally five: skin, superficial fat, muscle, deep fat, and bone (Figure 4). As this gradually occurs, bone remodelling and reduced facial vertical height, fat pad atrophy and repositioning will cause overall facial volume deficits that translate to subsequent facial tissue descent owing to a lack of anchorage and support.5
Figure 3. The changes with ageing.Figure 4. Cross-section of facial layers.
The depressor anguli oris, mentalis, and platysma muscles of the lower face also become stronger, adding to a descent and subsequent heavy appearance of the lower face. This often manifests to dentists as the ‘upside down’ smile appearance, with deep oral commissures.
Hyaluronic acid soft tissue filler
Hyaluronic acid fillers can be manufactured in different concentrations and crosslinked to varying degrees. These properties influence both their ability to bind water and expand, but also their viscosity and firmness. The ‘G prime’ of a filler relates to its elasticity and its resistance to deformation on force. A high G prime filler is firmer than a low G prime filler, is more resistant to vertical and lateral deformation under strain, and therefore has a greater capacity to lift and project tissues effectively. It is usually injected in the deeper, more static layers of the face, for example, supraperiostally in the cheek, chin, jaw or nose. A low G prime filler will compress better under force and, therefore, is considered ‘dynamic’. This makes it often more suitable for more superficial, mobile facial layers, such as the nasolabial folds, marionette lines, or lips.6
Neuromodulators of the face
Botulinum toxin is a neurotoxin that can be used to modulate muscle activity in the face for aesthetic purposes. When injected, botulinum toxin binds to nerve terminal receptors at a synapse junction, inhibiting the release of the neurotransmitter acetylcholine, thereby restricting muscle contraction.7
It can be of aesthetic benefit to inhibit the depressor muscles in the lower face and/or to reduce hyperactivity of the lip levators (levator labii superioris alequi nasi) in the case of a gummy smile reduction treatment.8
Dermal fillers: oro-facial considerations
Overall, there are numerous examples of cases in which lip or perioral treatment with fillers or neurotoxins are helpful to:
Improve lower lip support;
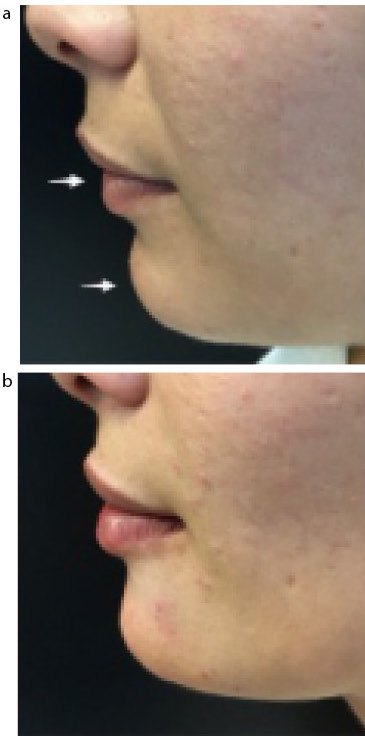
Reduce excess tooth show at rest (Figures 5 and 6);
Reduce increased gingival show upon smiling (caused by excess gingival tissue dento-alveolar compensation, or a hyperdynamic upper lip);
Disguise skeletal malocclusions through chin and lip augmentation.
Figure 5. Example of reduced tooth show at rest.Figure 6. (a) Before and (b) after pictures of profile balancing for a Class 2 occlusal/incisal/skeletal relationship.
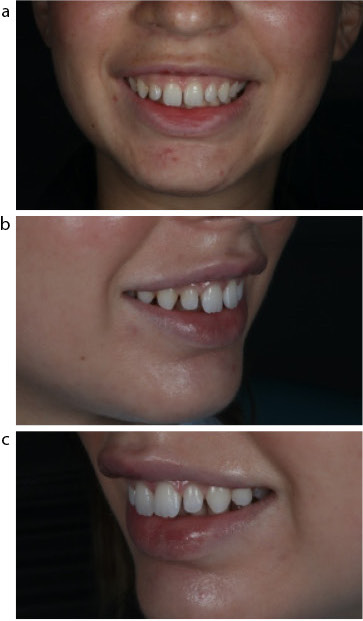
Case report of severe skeletal Class 2 jaw relationship, nasal dorsal hump and generalised dental spacing
This was a case of a young woman who attended two dental consultations relating to her gappy teeth. After outlining all the options, including composite bonding, porcelain veneers, orthodontics and/or orthognathic surgery, the patient opted for composite bonding. She had also been conscious of her side profile. She could not explain what she didn't like, but she knew that it looked imbalanced and convex. A profile balancing treatment involving her nose and chin (Figure 7), and her mid-face (Figure 8) was performed. Dental treatment was carried out before facial aesthetic treatment.
Figure 7. (a–d) External profile before treatment.Figure 8. (a–c) Internal profile before treatment.
Treatment provided
Dental treatment with composite bonding
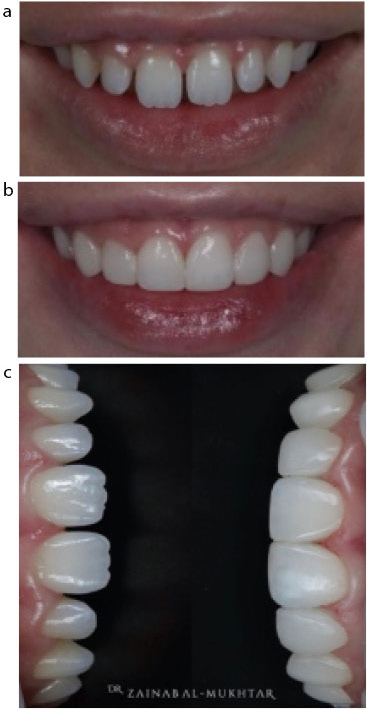
To mask the generalised spacing caused by her dento-alveolar discrepancies, teeth whitening was carried out followed by six composite veneers (Figure 9).
Figure 9. (a–c) Tooth whitening was carried out and six composite veneers were added.
Non-surgical rhinoplasty
After pre-treatment screening (vascular mapping) with colour Doppler ultrasound to visualise vessel depth (Figure 10), a highly viscous filler was injected suprachondrially on the nasal tip (midline) to rotate and elevate the under-projected tip and injected supraperiosteally on the radix (root of the nose) to disguise the dorsal hump. By influencing the point of light reflection to the centre of the nose, this improved the asymmetry visible on the frontal view, as well as reduced the perception of nasal convexity from the side profile.
Figure 10. (a,b) Pre-treatment vascular mapping with colour Doppler ultrasound.
Chin augmentation
An underdeveloped chin often makes the nose look larger. To achieve a less convex side profile, the chin was reshaped through filler augmentation on the pogonion and menton (on the periosteum) to improve inferio-anterior projection and elongation. This filler was chosen for both its lifting and projecting capacity, as well as its longevity. Chin augmentation with soft tissue filler also achieved a myomodulatory effect on the mentalis muscle. This was evidenced by the improvement in support of the lower lip, improved lip seal, and feedback from the patient on less mouth breathing (Figure 11). The patient was thrilled with this aesthetic and functional improvement.9
Figure 11. (a,b) Myomodulation and improved lip seal to disguise the Class 2 incisal relationship.
The pre-jowl sulcus was also injected with filler, using a microcannula, in the subcutaneous layer with a highly cohesive filler to blend together the jawline and the chin.
Gummy smile neurotoxin
Botulinum toxin was injected in the levator labii superioris alequi nasi, which is heavily involved in the elevation of the upper lip during smiling. Therefore, reducing muscle activity reduces upper lip elevation when smiling and minimises gum show (Figure 12). This treatment lasts between 3 and 4 months, so it requires upkeep if the patient is happy with the result. Patients who are suitable for this treatment must have an adequate amount of hyperaction of the levator muscle to produce adequate lip elevation.10
Figure 12. The reduction in gummy smile and the change in chin shape, with a better supported lower lip.
Cheek augmentation
Volume replacement with a dynamic hyaluronic acid filler in the deep medial cheek fat (DCMF) with a microcannula 25 g with a fanning technique;
Zygomatic arch was treated with periosteal bolus injections along the arch;
Zygomatic eminence was treated to increase projection of the OGEE curve, which is a significant ‘S’ shaped facial contour mostly appreciated from the oblique 45 degree perspective. When appropriately projected, this symbolises youth and femininity.
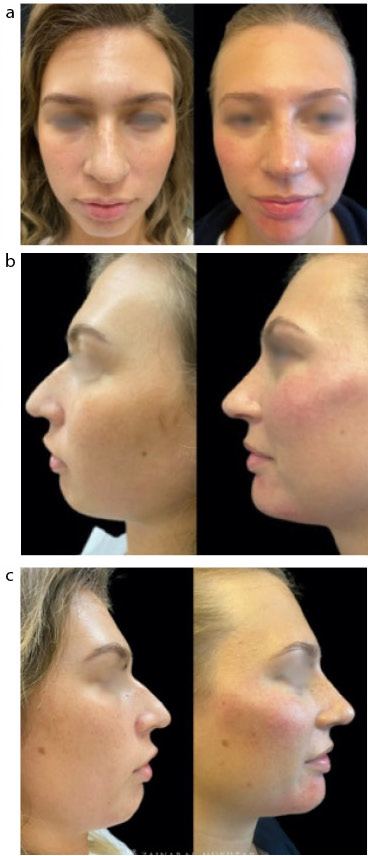
The feedback from this patient was overwhelmingly positive. She described newfound confidence in having photos taken of her at any angle and when smiling (Figure 13).
Figure 13. (a–e) After treatment.
Safety considerations
It is important that dentists are well versed in facial anatomy and undergo appropriate systematic training in injectable techniques that deliver safe and effective outcomes. While some of the vascular complications associated with soft tissue filler injections, are rare, they can be potentially serious. Augmenting certain facial features comes with greater risk, for example, the nose, the temple, and the piriform space. Dentists are considered to be among the most reliable professionals, in whom the public feels a sense of confidence regarding preventing and managing complications. Therefore, in addition to safe techniques, dentists should undoubtedly seek specific training in treating complications prior to embarking on delivering injectable treatments.
The beauty in combining
The intersection between dentistry and facial aesthetics brings about the beauty of combining both disciplines. Dentists have the unique ability to provide a holistic full-face approach to treatment, including the smile and facial transformation (Figure 14), notwithstanding that the smile is indeed a critical aspect of the face.
Figure 14. (a–c) Before and after comparisons of face.
For dentists, competence in assessing both the mouth, smile and the full-face, allows for the refinement of a very strong aesthetic eye, with a unique potential to easily zoom in to the mouth and zoom out to a full-face.
For patients, the experience of having a trusted dentist with whom a rapport and a trusting relationship have already formed is an excellent foundation for an enhanced patient experience in facial aesthetics, whereby the level of trust can only be elevated further and with ease. The psychosocial benefits of facial aesthetics can be life-changing, and alongside smile aesthetics, the impact can be truly profound.