Fahl N, Denehy GE, Jackson RD Protocol for predictable restoration of anterior teeth with composite resins. Pract Periodontics Aesthet Dent. 1995; 7:13-21
Feilzer AJ, De Gee AJ, Davidson CL Setting stress in composite resin in relation to configuration of the restoration. J Dent Res. 1987; 66:1636-1639 https://doi.org/10.1177/00220345870660110601
Burke FJ, Shortall AC Successful restoration of load-bearing cavities in posterior teeth with direct-replacement resinbased composite. Dent Update. 2001; 28:388-398 https://doi.org/10.12968/denu.2001.28.8.388
The art of clinical shade matching of resin-based composite materials Dipesh Parmar Louis Mackenzie Stephen J Bonsor Aesthetic Update 2025 1:3, 113-120.
The present article is the second in a series of three on shade matching in restorative dentistry. The first article provided an overview and general advice on shade taking. This article goes on to discuss what factors should be considered when choosing the most appropriate shade guide in relation to resin-based composite materials. It offers practical advice on how shade guides may be used to best effect in determining an optimal match with respect to optics between the dental hard tissues and resin-based composite products to achieve highly natural imperceptible results when working in the aesthetic zone.
CPD/Clinical Relevance:
The art of shade matching is a fundamental clinical skill in restorative dentistry to ensure that the best possible aesthetic outcome is achieved when working with resin-based composite materials.
Article
Modern dental materials must have advanced colour-matching properties to satisfy patient and professional demand for high-quality natural and lifelike restorations. Resin-based composite is used extensively as a direct aesthetic restorative material, both in the aesthetic zone and the posterior regions of the mouth. There are many types of this material available commercially, which is outwith the scope of the present article; however, in order to understand their clinical handling, interested readers may wish to refer to the article by Bonsor that covers the material science of resin-based composites, their advantages and shortcomings.1 A thorough understanding of the material science is crucial to effectively practise restorative dentistry, and thus achieve the best outcomes.2
When working in the aesthetic zone, a layering resin-based composite product would be the product choice of most clinicians. Essentially, these systems are composed of resin-based composites with differing optical properties, resembling natural dental enamel and dentine, so allowing the defect in the tooth to be reconstructed in layers for an optimal aesthetic result. Apart from the excellent aesthetics that may be obtained by the skilled use of these products, another advantage is that the material may be bonded to the dental hard tissues. This means that a conservative technique may be employed because sound tooth tissue does not need to be removed as traditional resistance and retention form in the cavity is not a consideration.
The present article follows on from the first article in this series that explained the fundamentals of shade matching3 and will concentrate on shade matching when direct restorations are being constructed using resin-based composite.
Shade guides for matching resin-based composite materials
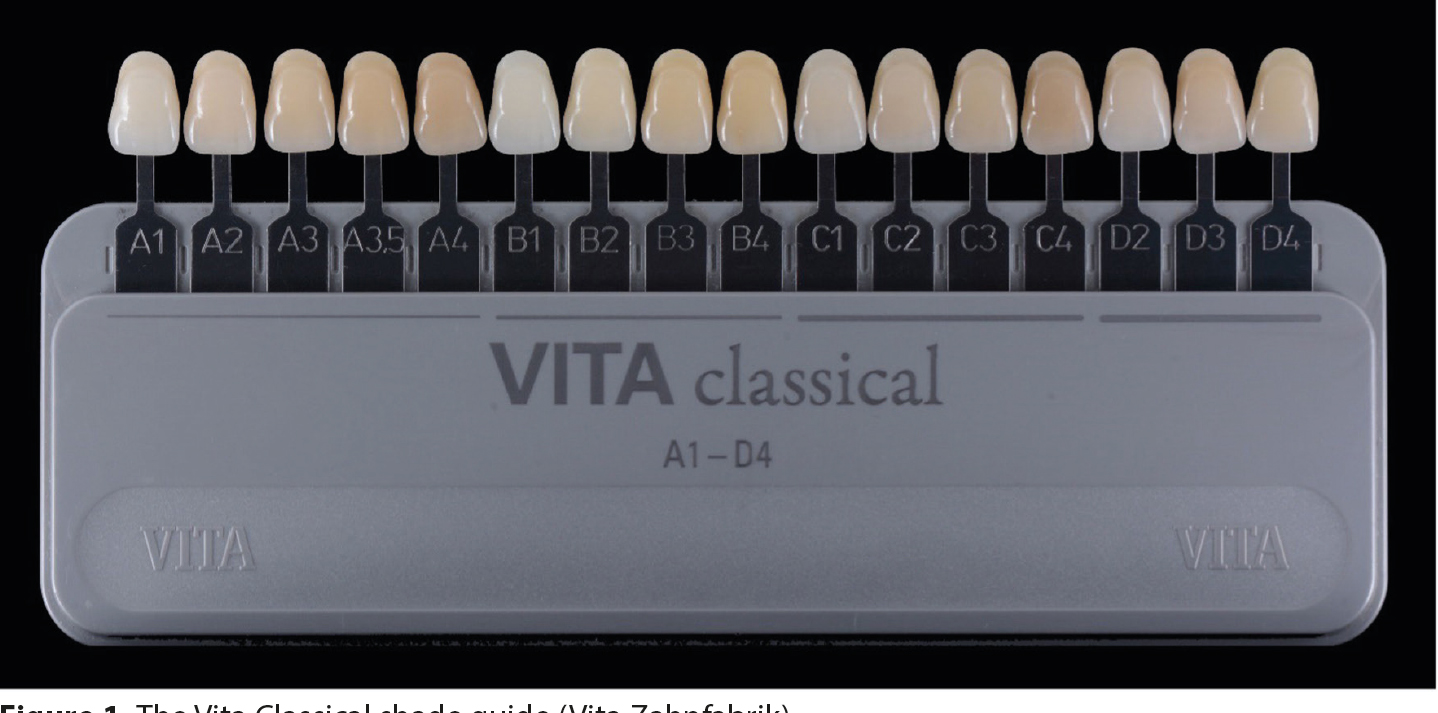
Traditionally, a shade guide, which is a range of shade tabs, was used by the dentist to determine the required shade of material to be employed by matching the shade of the natural tooth to the closest matching tab. The best known and most widely used shade guide is the Vita Classical system (Vita Zahnfabrik, Bad Säckingen, Germany)(Figure 1).
Figure 1. The Vita Classical shade guide (Vita Zahnfabrik).
This shade guide consists of 16 shade tabs arranged with respect to their different hues (A–D) and in varying chroma levels (1–4). The vast majority of human teeth match the ‘A’ shades of the Vita Classical system. Originally, this particular shade guide was introduced in 1956 to match the newly introduced ceramics. The ability to choose the correct shade of these materials using this guide was hampered as the shade tabs are composed of acrylic, and trying to match dissimilar materials accurately is virtually impossible. Furthermore, the colour ranges and distributions within each tab is not natural. Natural teeth have many optical nuances that must be matched to ensure an optimal result, as discussed in the first article of this series (Figure 2).3
Figure 2. A clinical photograph illustrating the optical complexities of natural teeth compared with a homogeneous shade tab.
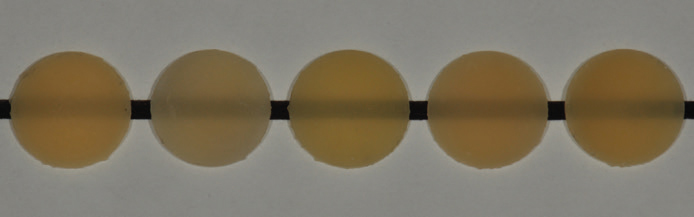
Many resin-based composite products on the market recommend the use of the Vita Classical shade guide when selecting the shade of the material to be used. Unfortunately, there can be significant variations in the hue, value, chroma and opacity of different commercially available products, which is demonstrated in Figure 3.
Figure 3. Five samples of A3 resin-based composite of a 0.5-mm thickness that demonstrate the significant variances in hue, value, chroma and opacity between the products.
This lack of consistency between different resin-based composite manufacturers for a particular shade, means it is not possible to use the Vita Classical shade guide predictably. Therefore, when shade matching resin-based composite to natural tooth tissue, a shade guide made of said material should be used. These may be divided into two types, one supplied with the product and the other is custom made.
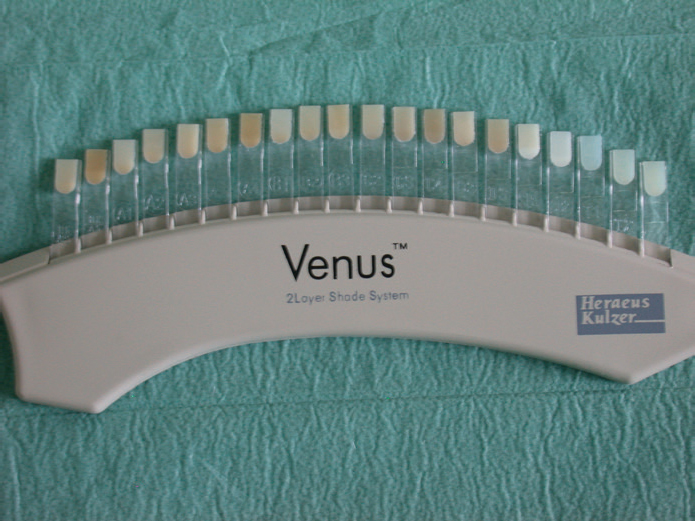
The shade guide supplied with the product may be constructed of simple tabs, similar to the Vita Classical shade guide, composed of the resin-based composite material itself, but consisting of homogeneous shade tabs, for example, A1, A2, A3 etc (Figure 4).
Figure 4. An example of a shade guide where the tabs are composed of the resin-based composite material, Venus (Kulzer, Basingstoke, UK).
Other layering resin-based composite products offer a more advanced shade guide consisting of ‘shells’ composed of enamel shades, which may be fitted over the ‘cores’ made with dentine shades. This method helps the clinician arrive at a more predictable choice of shade of material.
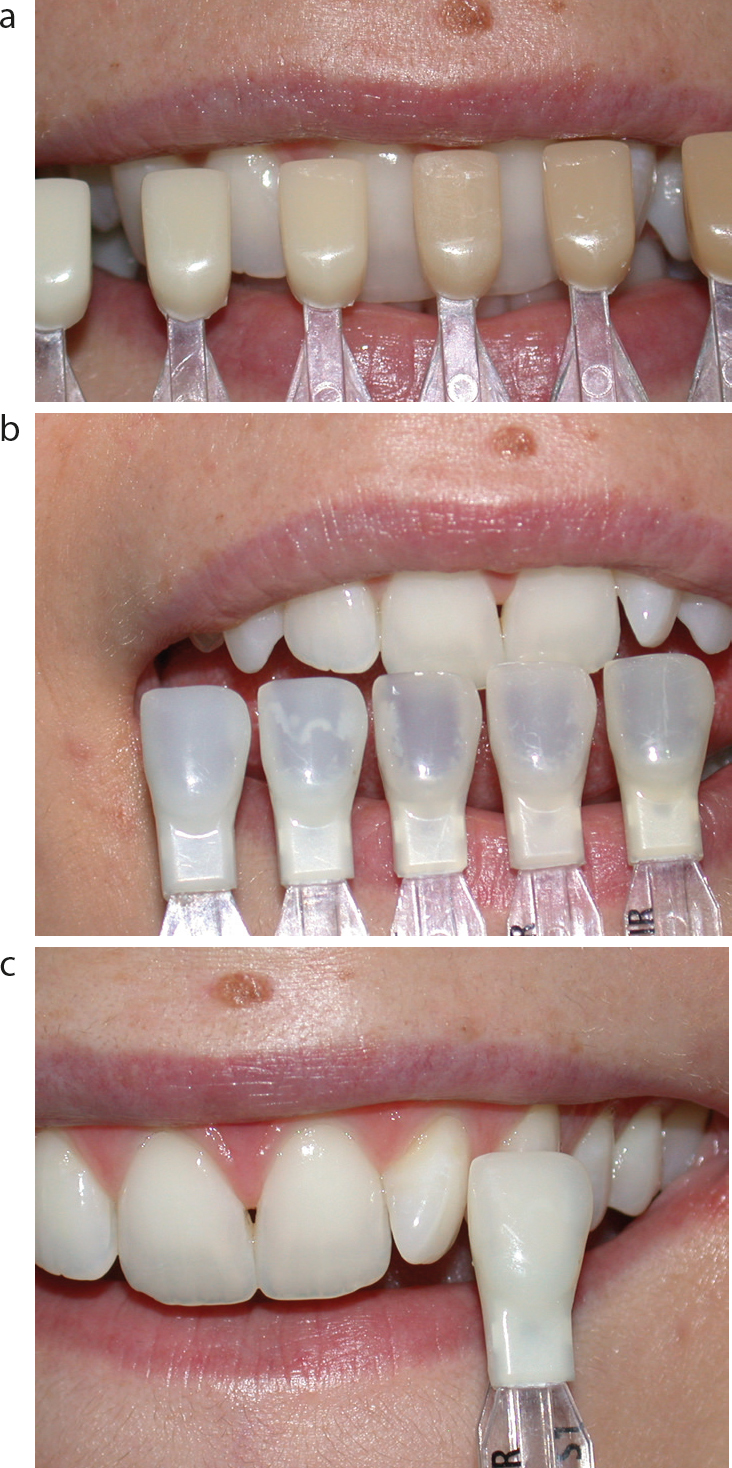
One such product is Miris 2 (Coltène Whaledent, Altstatten, Switzerland) (Figure 5).
Figure 5.
(a–c) The supplied shade guide of ‘enamel’ shells and ‘dentine’ cores provided for the purposes of shade matching with Miris 2 (Coltène Whaledent), a layering resin-based composite product. The dentine shade is taken from the cervical region of the tooth and the enamel shade, incisally as shown. The shell is then placed over the core, thus giving the clinician an accurate idea of the final appearance of the restoration.
For those products that are not supplied with such a shade guide, other commercially available products are available that allow shells mimicking dental enamel to be made from any resin-based composite. Figure 6 shows one such product in which the ‘enamel’ shell can be used as the enamel shade tab, or may have the dentine shade placed over it to provide a guide as to the final restoration. Equally, the dentine shade tab may be used on its own.
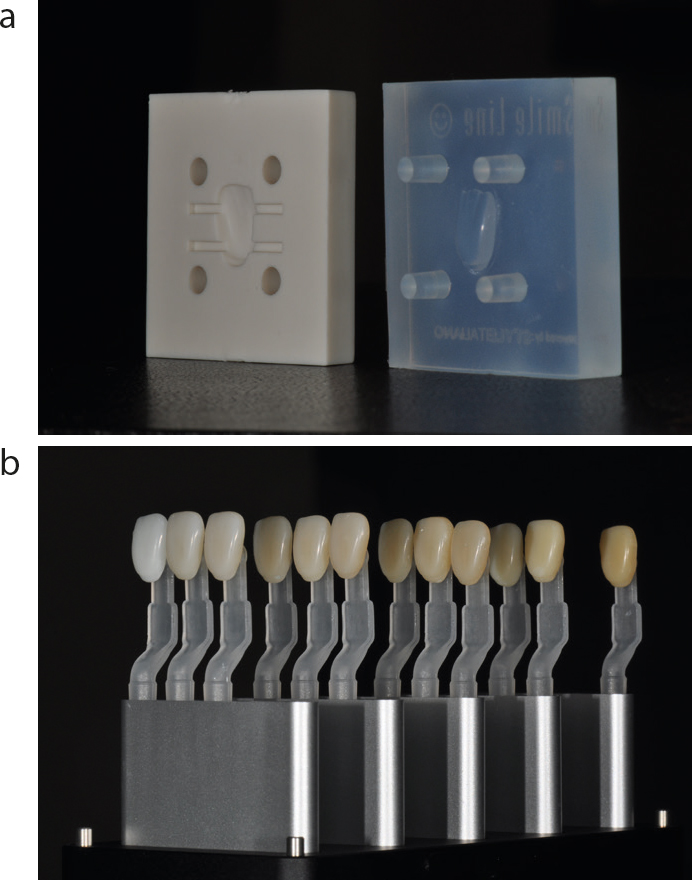
Figure 6.
(a,b) A bespoke shade guide consisting of ‘enamel’ shells and ‘dentine’ cores may be constructed using a commercially available product, StyleItaliano (www.styleitaliano.org/).
The recommended shade-taking protocol when using such a system can be seen in Figure 5. The shade of the dentine is determined in the cervical region of the tooth where dentine is more plentiful and dental enamel thinnest, and similarly the enamel shade is gauged by comparing the ‘shell’ with the incisal edge of the tooth. With a small amount of glycerine between the core and shell to remove the air barrier, which affects the passage of light through the system and hence its optical properties, the final shade can be readily compared with the tooth. This provides a more predictable method of matching shades when working with layering resin-based composite products.
A custom-made shade guide can be constructed in surgery using the material and micro-brushes as handles4 and is shown sequentially in Figure 7.
Figure 7. The method of construction of a custom-made shade guide. (a) A celluloid crown form is selected. (b) Its cervical portion should be removed with a pair of scissors or crown shears. (c) The crown form is filled with resin-based composite except for the central area and light cured. (d) This hollow central area is filled with more resin-based composite, and a micro-brush is inserted into the unset material. (e) This last increment is light-cured, and the celluloid crown form is removed. (f) The formed shade tab may then be trimmed and polished.4
As with wallpaper and paint, there may be variations between batches of material, so strictly speaking, such a shade guide should be constructed with each new batch of resin-based composite product. However, it is acknowledged that the difference may be so slight as not to warrant the extra expense in terms of time and material.
The use of clinical photography to facilitate shade determination
Some operators advocate the use of a shade map drawn from the pre-operative clinical photograph. This technique, however, may introduce errors and inaccuracies into the drawing. Furthermore, when the contralateral tooth is being drawn to create the shade map, the image must be mentally flipped when determining the placement of the shades and effects. Confusion may therefore occur during the clinical placement of the resin-based composite material. For this reason, the use of clinical photography only is recommended because it can be a useful tool in shade determination, especially in aesthetically demanding clinical situations. The design of restoration shape, surface texture and polychromatic colour may be enhanced by the use of close-up clinical photography, which may then be used as a shade map. Figure 8 illustrates the protocol.
Figure 8. The use of a pre-operative photograph as a shade map. The process is thus described: Step 1: A quality pre-operative photograph should be taken with minimal light reflections. A cross-polarized image can be used. Step 2: The image should be rotated 180° to simulate the supine position of the patient during treatment. Step 3: The image is then flipped horizontally. This has the effect of putting the being replicated in the position of the tooth being restored. Step 4: The image should then be manipulated via increasing contrast, changing the exposure and cropping to leave an image with internal effects easily visible. Step 5: The digital map may then be used to build the restoration.
Other practical tips on how clinical photography can be used in the determination of shade include the following.
Increasing the contrast of clinical photographs using image manipulation software allows the identification of subtle colour characteristics, as often seen in the incisal third of maxillary anterior teeth.
Neutral backgrounds (black/white/mid-tone grey) are recommended for clinical photography.
Black and white photography, or monochrome conversion of colour images may be used to determine correct values.
Twin flashes, rather than ring/point flashes, allow better assessment of surface texture details, especially transition lines.
Slightly underexposed images may also be used to study surface texture.
Digital single-lens reflex (DSLR) cameras/macro lenses with standardized settings are recommended for consistent colour reproduction (Table 1).
Camera/flash
Manual
Shutter speed
1/200 second
Aperture
F:22–F:32
ISO
Lowest possible, e.g. 100
White balance
Natural daylight, 5500K
Clinical determination of the shade of resin-based composite products in the aesthetic zone
The fundamentals and general principles of shade matching were explained in depth in the first article in this series, which the reader may wish to review.3 The remainder of the present article will be devoted to shade matching resin-based composite in the anterior and posterior regions.
General practical tips
Teeth should be cleaned to remove extrinsic stains using a brush and a slurry of flour of pumice and water. Avoid the use of prophylaxis paste as it will have a detrimental effect on the subsequent bonding procedure.
Resin-based composite restorations, being sensitive to moisture, should be placed under rubber dam, the most effective moisture control technique. The shade should be determined prior to rubber dam placement as the teeth will quickly dehydrate and so lighten in shade.
If possible, ideally a shade guide constructed of the selected product should be used, or custom-made as previously described. Which failing, the operator should follow the instructions of the manufacturer as regards the recommended shade guide. Where the tooth to be restored closely matches a specific Vita Classical shade, analogous resin-based composite enamel and dentine shade tabs of varying thickness may be used to determine the optimal translucency and opacity for layered restorations. This is determined in some systems by the use of a ‘recipe wheel’ (Figure 9).
The three or four closest shade tabs should be selected before beginning a process of elimination.
The middle third of the subject or adjacent tooth should be used to determine basic shade, as colour typically ranges from the cervical to the incisal areas (a general decrease in chroma and hue is usually seen).
Translucency is best evaluated using a black background. A photographic contraster may be used for this purpose (Figure 10).
Where the closest Vita Classical shade has slight chromatic differences from the natural tooth, customized shade tabs featuring different combinations of enamel and dentine shades in standardized thicknesses may be used for precise shade selection (Figure 6).5
Cavity size, shape and position should be studied, and the relative thicknesses of residual dental enamel and dentine should be measured.
A small amount of material of the selected shade should be placed onto the unetched surface of the tooth and light cured. Many products undergo a shade shift on photopolymerization, meaning that the shades between the uncured and cured material may differ. The clinician will be better able to determine the final shade more accurately once the material has been cured. The cured material may then be easily detached from the surface of the tooth (Figure 11).
Deeper resin-based composite layers should be shaped to conform to the anatomy of natural dentine (Figure 15).
As a general rule, The enamel layer should be no thicker than 0.5 mm (Figure 15).
Surface gloss (the ability of the tooth surface to reflect light) has a significant impact on the optical properties of teeth, and many layering resin-based composite materials are designed to allow quick and easy polishing to a high, naturally appearing surface lustre (Figure 15).
During restorative procedures, full dehydration is reported to occur after approximately 30–40 minutes. As it can take up to 2–3 days for teeth to fully rehydrate, it is important to monitor restorations over time to perfect layering techniques (Figure 12).
No deviation should be made from pre-operative shade decisions because teeth lighten during restorative procedures.
Classic polychromatic layering technique6 starts with the placement of an enamel ‘shell’, which may be easily formed using a palatal silicone template constructed from a pre-operative wax-up (Figure 13e).
Opaque dentine lobes are then restored and shaped depending on the desired optical effect (Figure 13f).
Based on the pre-operative colour map, specialized tinted ‘effect shade’ flowable consistency composites such as Creative Color (Cosmedent, Chicago, USA) are then applied and light cured on the final dentine layer (Figure 13g).
The labial enamel layer is then placed before carrying out shaping, finishing and polishing procedures (Figure 13h). The labial enamel can be a chromatic enamel shade, an achromatic enamel shade, or layering of both.
Figure 9. An example of a ‘recipe wheel’ advocated by certain manufacturers, in this case, 3M ESPE, to guide the clinician having chosen a single shade using the Vita Classical shade guide, on which resin-based composite shades should be used to construct the layered restoration.Figure 10.
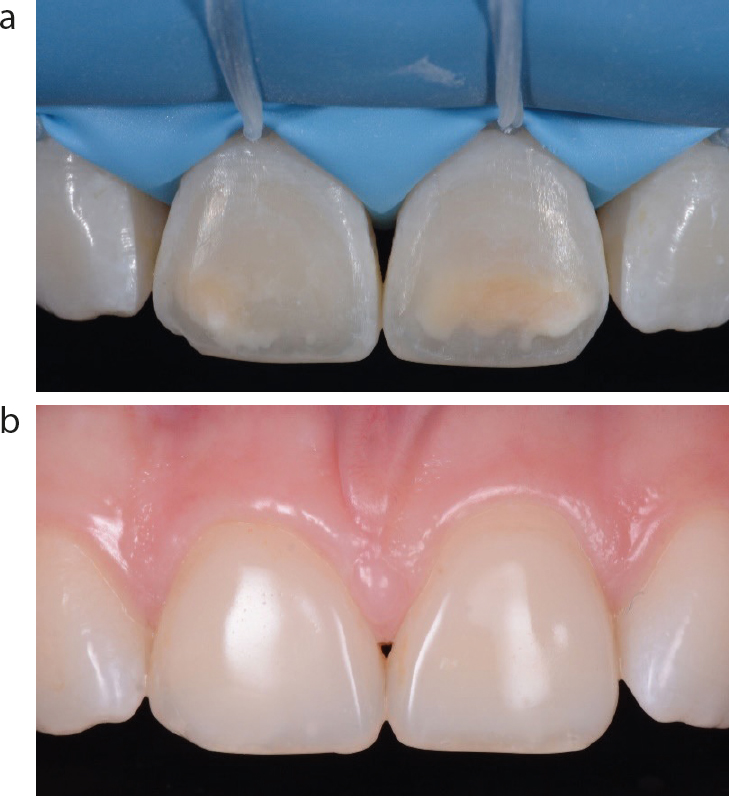
(a) A contraster is used in clinical photography to provide a black background to enhance the appearance of the restoration, as illustrated by (b), especially with respect to translucency.Figure 11. Various samples of resin-based composite material have been placed on the tooth and the adjacent tooth to determine shade and then light cured. Cross-polarized photography assists in shade selection by removal of the specular reflections.Figure 12. Two images illustrating the importance of monitoring restorations over time to perfect layering techniques. (a) The pre-operative view and (b) the 8-year (untouched) recall of the patient who underwent the provision of Renamel Microfill (Cosmedent) resin-based composite labial veneers on the upper central teeth.Figure 13.
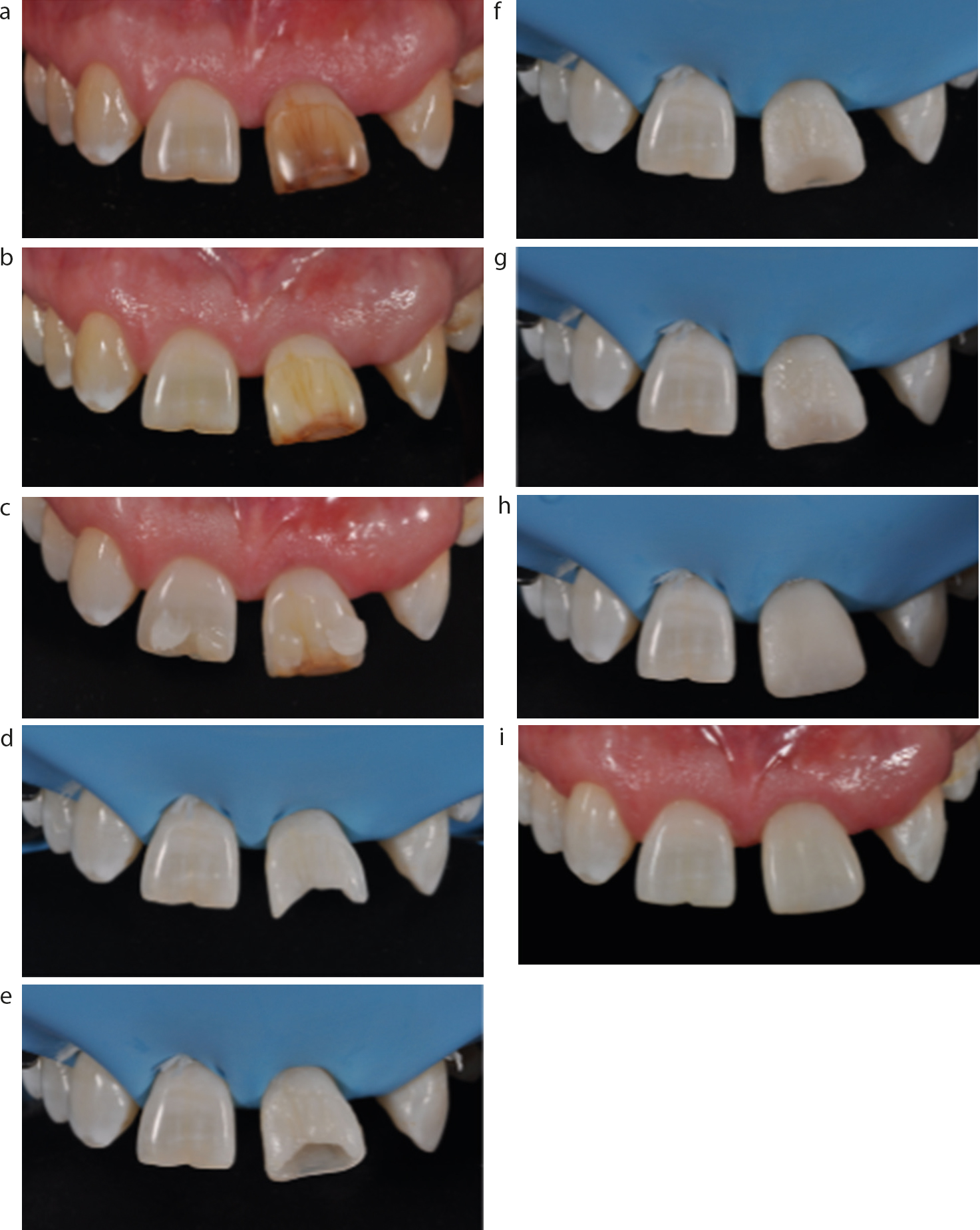
(a–i) A case illustrating the aesthetic restoration of UL1, which was first bleached and then restored using a three-shade technique using resin-based composite.Figure 14.
(a–c) Although monochromatic restorations have their limitations, aesthetically high-quality restorations can be produced.Figure 15.
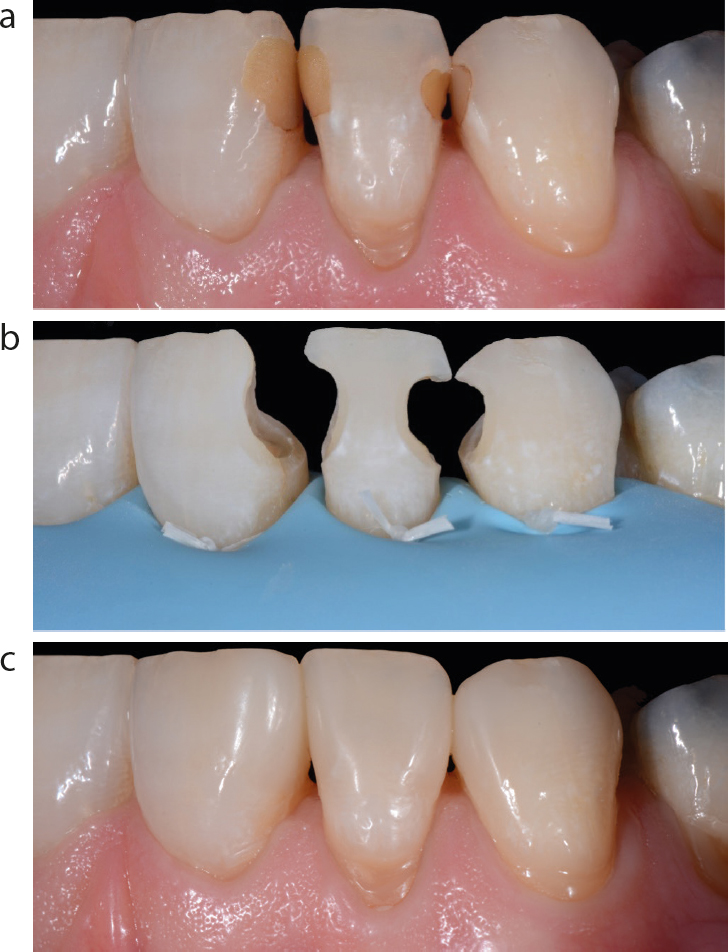
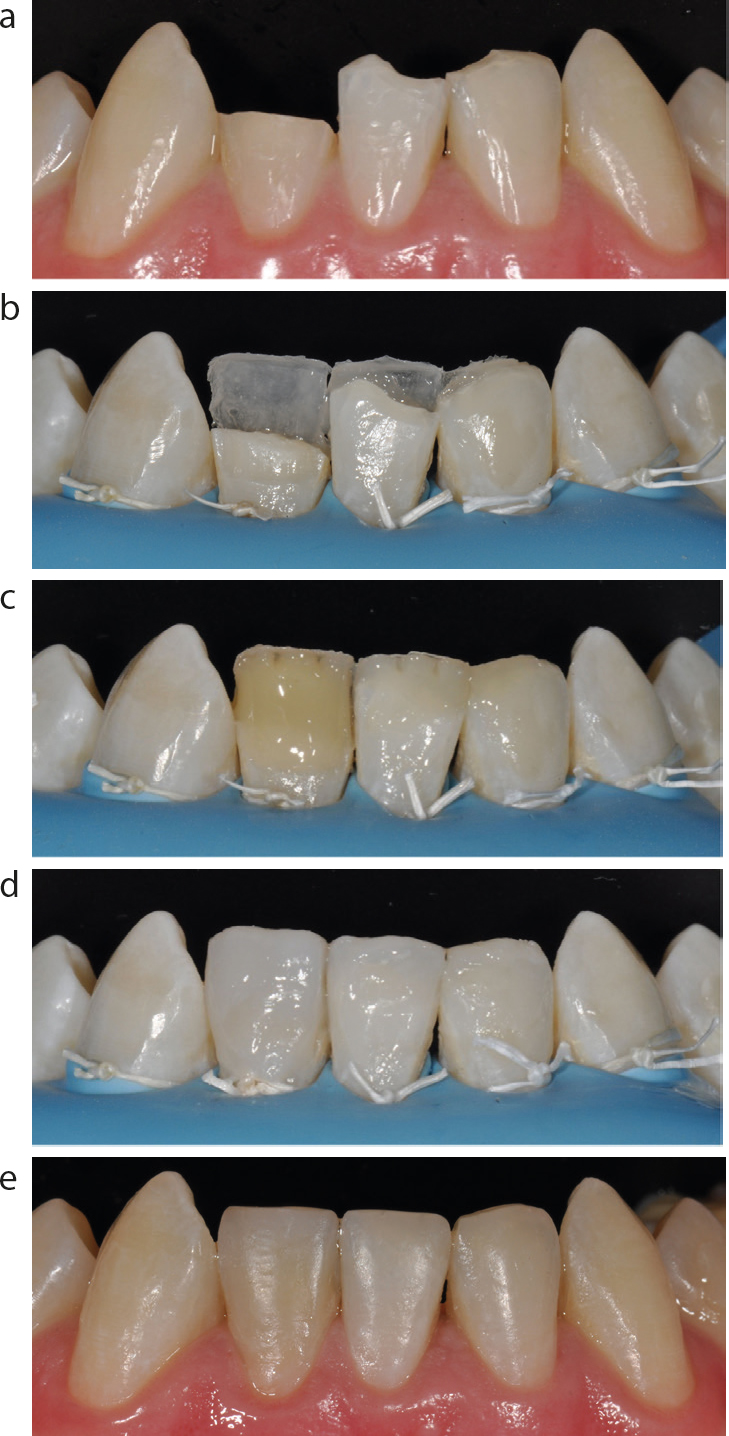
(a–e) Three lower incisor teeth were restored in resin-based composite using a two-shade technique.
Shade matching with resin-based composite placement techniques
There are three placement techniques when providing resin-based composite restorations in the aesthetic zone. These are the use of a single shade, two shades (enamel and dentine) and three shades or more (enamel/dentine/effect shades). These techniques are now considered.
Single-shade technique
The traditional technique involved the placement of a single shade of material. Many resin-based composite systems have enhanced blending properties, which allow most damaged teeth to be restored with a single shade of resin-based composite. This is especially so when restoring small cavities (for example, Class III), teeth with uniformly opaque enamel (for example, in young patients) or when providing multiple restorations to restore severe non-carious tooth surface loss. This technique is used in contemporary practice when aesthetics are not considered to be a priority for the patient because the procedure being quicker to perform is less costly in terms of time and financial expense. A case by means of illustration is pictured in Figure 14.
Two-shade technique
Dental enamel and dentine have different structural characteristics so influencing their optical properties. Dental enamel is translucent and allows some light to pass through into the more opaque dentine, which absorbs light and reflects subtle colours back to the observer through the translucent dental enamel. The final tooth colour is determined by a combination of the reflective, absorptive and refractive properties of the dental hard tissues.
As an exact single-shade match in dentistry is rare, layered combinations of translucent and opaque layering resin-based composite shades may be used to mimic the optical properties of dental enamel and dentine. It is recommended that the minimum number of layers be applied to achieve optimal aesthetic integration. Tints may be used to add further characterizations to the restorations in an efficient manner.5 This technique is demonstrated in Figure 15.
Three-shade + technique
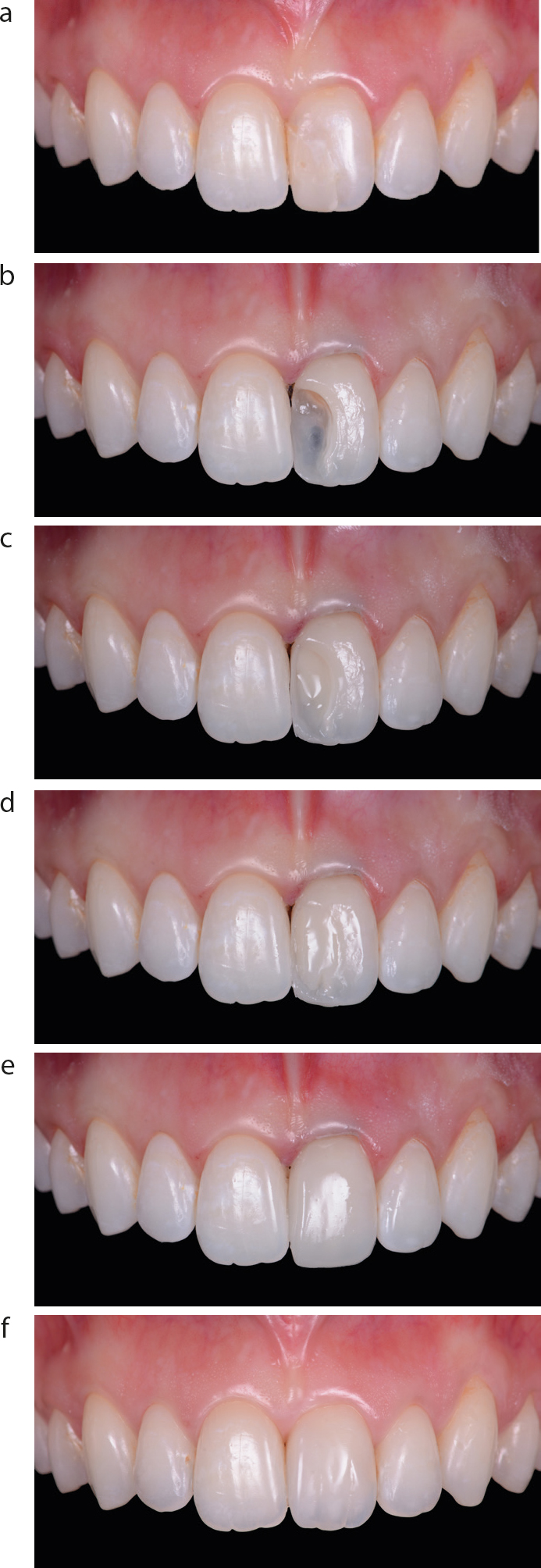
This technique is an enhancement on the two-layer technique and should be employed in cases when aesthetics is of the highest priority and importance. In the same way that a natural tooth is composed of an outer covering of dental enamel with a dentine core, the three-shade technique involves a specific palatal enamel layer to be laid down (a different shade to the labial enamel), cored with a dentine shade with opaquers and tints, and then the final enamel layer(s) placed on the labial surface, so mimicking the structure of a natural tooth. Such a case is illustrated in Figure 16.
Figure 16.
(a–f) An example of a clinical case restoring UL1, using a three-stage + technique.
Many current commercially available materials can be used posteriorly, although the clinician has a responsibility to ensure that their chosen product is indicated for such a situation. The potential problems that arise from the effects of polymerization shrinkage stress are more relevant in this situation. The type of resin-based composite will determine its clinical placement1 in that so-called bulk-filled restorative materials may be placed in large increments while the more traditional products need to be placed incrementally so as to ensure full cure of the material while reducing the polymerization shrinkage stress by paying attention to the configuration or C factor.7
Traditionally, function was considered more important than aesthetics in the posterior region and so products were developed with enhanced mechanical properties, such as the packables, which were available in only a few shades. This meant there was a decreased importance attached to accurate and exact shade matching. In fact, there is a school of thought that advises that there should be a slight mismatch between the shade of the restorative material and the tooth tissue.8 This will facilitate the future removal of the restorative material should this be required. If the shade match is excellent, then this is more challenging with the result that more sound tooth tissue is removed than would be desirable during cavity preparation.
That said, should there be a demand by the patient or indeed the artistic clinician, then excellent aesthetics can be provided with imperceptible margins between the restorative material and the dental hard tissues. Tints, effects and stains are provided with some kits and available to buy as products in their own right as mentioned earlier. An example of what can be achieved when restoring a molar tooth is shown in Figure 17f.
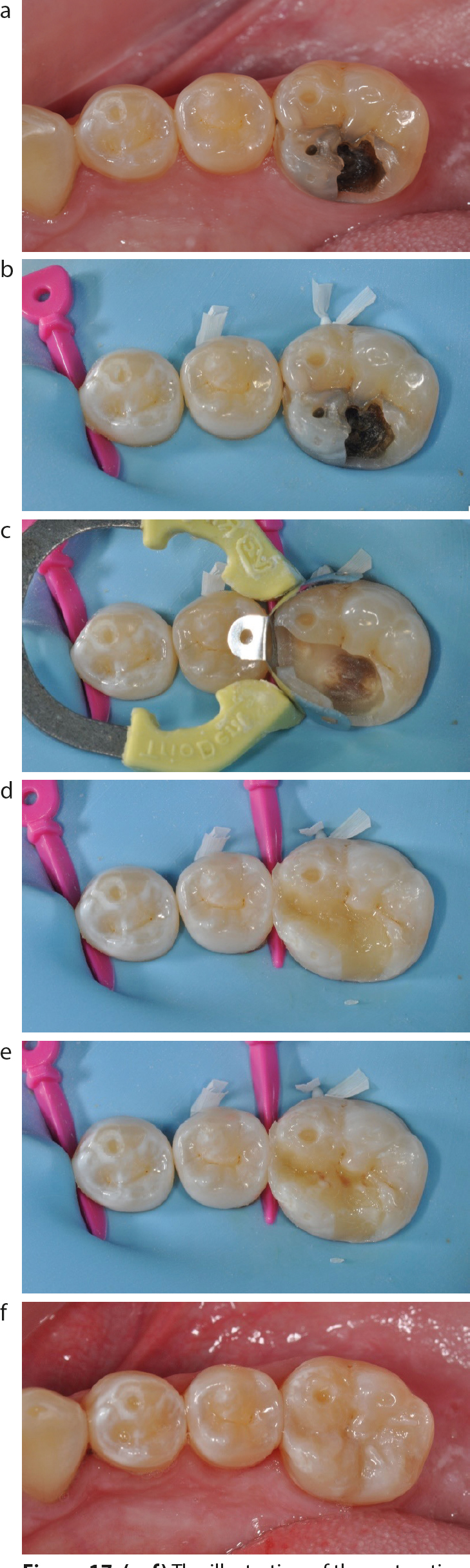
Figure 17.
(a–f) The illustration of the restoration of LR6, using a resin-based composite material, as described in the text.
Practical tips for posterior composite restorations using a resin-based composite material
The pre-operative shade is selected using the techniques described previously and prior to isolation (Figure 17a). A rubber dam should be placed prior to cavity preparation (Figure 17b). Restorations composed of metal alloy, if present, should usually be removed entirely to avoid the risk of ‘shine through’, and the carious lesion managed appropriately. In the case of a cavity involving the approximal surface of the tooth, a sectional matrix system should be used (Figure 17c). After etching, adhesive resins are applied and light-cured according to the manufacturer's instructions. Opaque dentine shades may be used to block out darkly stained cavity floors (Figure 17d). The final enamel layer of the material may be quickly and easily shaped to restore occlusal anatomy (Figure 17e). A tinted flowable resin-based composite product, as mentioned earlier, may be applied to define occlusal pits and fissures. Excess ‘fissure stain’ should be blotted with a dry micro-brush before light curing. The advanced aesthetic and handling properties of a layering resin-based composite product enables the quick, efficient and predicable restoration of posterior teeth (Figure 17f).
Conclusion
In order to achieve natural imperceptible restorations constructed in resin-based composite, the treating clinician needs to consider which shade guide they use and how they use it. Careful shade selection, perhaps using clinical photography and the tips described in the present article, will pay dividends in achieving the desired goal. The final article in the series will discuss shade matching in relation to indirect restorative materials.