Mackenzie L. Technique Tips: How to make a customized shade guide. Dent Update. 2019; 46:396-397
Poljak-Guberina R, Celebic A, Powers JM, Paravina RD. Colour discrimination of dental professionals and colour deficient laypersons. J Dent. 2011; 39:e17-22 https://doi.org/10.1016/j.jdent.2011.09.008
Alomari M, Chadwick RG. Factors influencing the shade matching performance of dentists and dental technicians when using two different shade guides. Br Dent J. 2011; 211 https://doi.org/10.1038/sj.bdj.2011.1006
Capa N, Malkondu O, Kazazoglu E, Calikkocaoglu S. Evaluating factors that affect the shade-matching ability of dentists, dental staff members and laypeople. J Am Dent Assoc. 2010; 141:71-76 https://doi.org/10.14219/jada.archive.2010.0023
Samra APB, Moro MG, Mazur RF Performance of dental students in shade matching: impact of training. J Esthet Restor Dent. 2017; 29:E24-E32 https://doi.org/10.1111/jerd.12287
With a move in contemporary restorative dentistry towards the provision of tooth-coloured restorations, the ability of the clinical team to achieve imperceptible shade matching between the (direct or indirect) restorative material and the dental hard tissues is highly desirable. The present article provides an overview of the physics of light, and how colours are perceived by the human eye. It then discusses the factors that affect the optical properties of natural teeth and dental restorative materials alike, and provides tips on how the clinician can achieve best results when ‘taking the shade.’
CPD/Clinical Relevance: The art of shade matching is a fundamental clinical skill in restorative dentistry to ensure that the best possible aesthetic outcome is achieved.
Article
Modern tooth-coloured restorative materials, especially those to be used in the aesthetic zone, must have the ability to mimic the dental hard tissues in terms of optical properties to satisfy patient and professional demand for high-quality imperceptible restorations. Accurate colour matching remains one of the most challenging tasks in clinical dentistry. In order to achieve the most predictable aesthetic outcomes, it is essential to have a detailed understanding of the fundamental optical properties of natural teeth and those tooth-coloured dental materials employed to restore lost dental hard tissue. The present article, the first in a series of three, concentrates on the interaction between visible light and natural dental tissues, and how the human eye may perceive this interaction. Furthermore, it will offer some general practical advice and tips on how to achieve best results especially when taking a shade in the aesthetic zone.
The physics of light and colour perception in humans
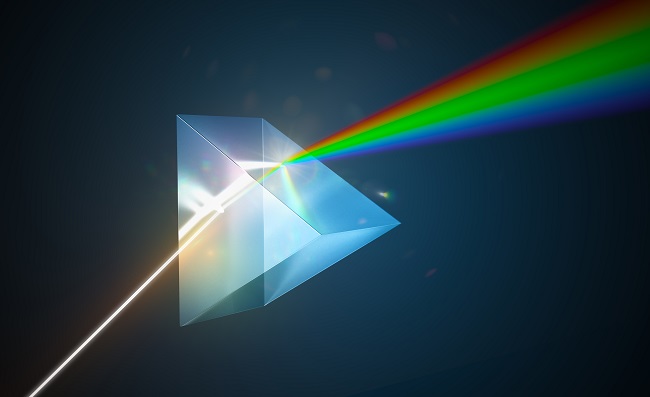
Visible light is electromagnetic radiation at wavelengths in the range of 400–700 nm. If light is transmitted through an optical prism, the light is refracted, varying with the wavelength of the light, thus white light is split into its constituent colours. Blue light has a shorter wavelength and a higher refractive index than red light, i.e. it deviates more (Figure 1).
Figure 1.
The phenomenon of dispersion, whereby a prism has divided white light into its component colours of the visible light spectrum.
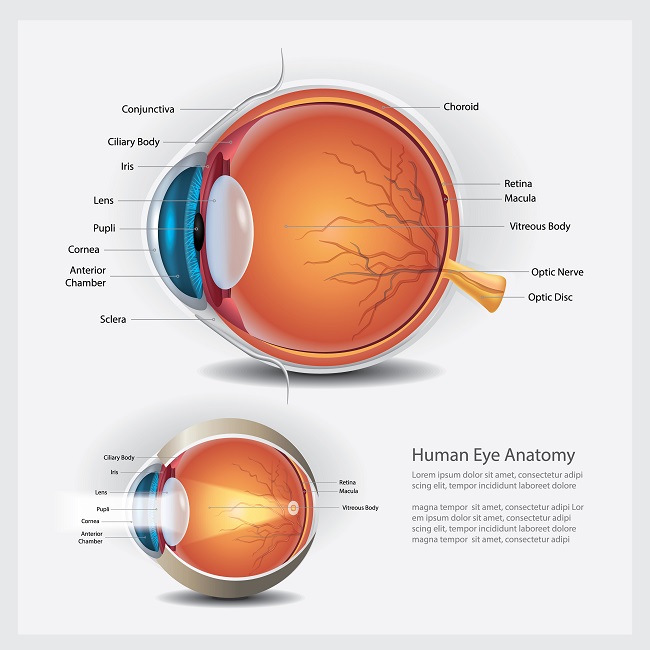
Similarly, the lens in the human eye uses refraction to redirect light onto the retina, the light sensitive tissue at the back of the eye. The retina contains photoreceptor cells that can distinguish millions of different colours and are efficient at detecting even small colour differences between two objects (Figure 2).
Figure 2.
Diagram showing the main structures of the eye. When visible light enters, it is refracted by the lens and redirected onto the retina.
There are broadly two types of cells in the human retina, namely rods and cones. Rods are highly light-sensitive and determine the intensity of light or light and dark, thus providing vision in a range of light levels, especially in low light conditions. Rods perceive light in the black/white/grey scale and number some 120 million.
By comparison, there are approximately 6 million cones in a human eye and they are most receptive to colour, but are less sensitive than rods. They, therefore, require brighter illumination and tire quickly. There are three cone types in humans, hence the term ‘trichromatic’ to describe normal human vision. These cells are sensitised to short, medium and long wavelengths, namely the colours blue, green and red in a proportion of 10%, 30% and 60%, respectively.
Description of colour
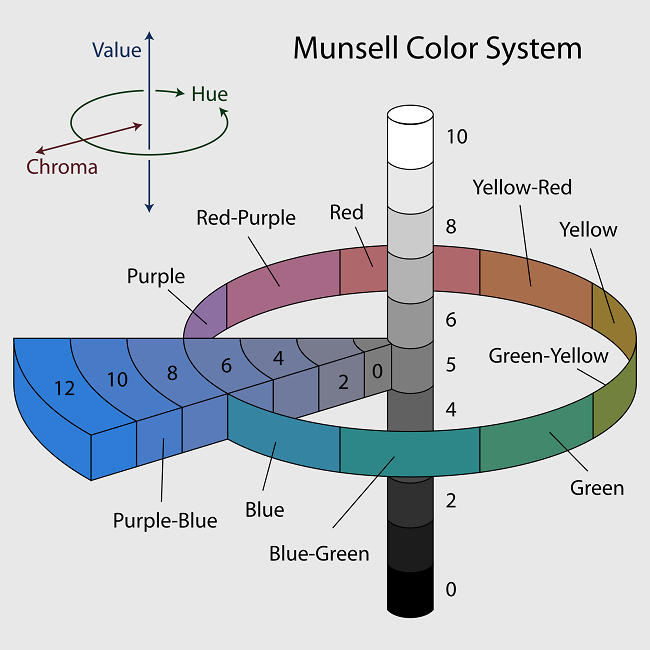
The ‘Munsell colour system’ was proposed in 1929 and separated colour, for the first time, in terms of three independent, yet perceptually uniform dimensions. These parameters are hue, which is the name of the intrinsic colour, chroma, which denotes colour saturation or intensity, and value, the lightness or darkness. In addition, value also involves brightness and the amount of light reflected back to the observer. The Munsell colour system can be seen diagrammatically in Figure 3.
Figure 3.
A diagrammatic representation of the Munsell colour system. The circle (of colours) denotes the hues, the central rod denotes the values (from 0 to 10), and the wedge represents the chromas. Courtesy of Jacob Rus (available at: https://commons.wikimedia.org/wiki/File:Munsell-system.svg).
Munsell was also the first to illustrate the colours systematically in three-dimensional space, which has been supported by the extensive measurement of visual responses in humans. Apropos of Munsell's colour system, human natural teeth and tooth-coloured restorative materials are generally referred to as ‘shade’ based in terms of their colour. The most commonly used shade guide is shown in Figure 4. Table 1 relates the work of Munsell with the shade-based colour determination that is used in dentistry.
Figure 4.
The Vita classical (Vita) shade guide, the most commonly used shade guide.
Table 1.
The Munsell colour system as applied to human teeth and tooth-coloured restorative materials.
The name of the intrinsic colour Corresponds to the wavelength of the reflected lightThe hue of teeth is mainly determined by the colour of the dentine, which lies predominantly in the yellow part of the spectrum Saturation or intensity of a specific colour As shade numbers increase, teeth and restorative materials become more chromatic and generally darker/yellower Lightness/darknessBrightnessThe amount of light reflected back to the observer This is the most influential colour dimension and makes up 70% of the colour of a tooth or restorative material
Factors affecting the optical properties of natural teeth and dental restorative materials
There are many factors, combined with their complex interaction, that affect the optical properties of natural teeth and those tooth-coloured dental materials that are employed to restore lost dental hard tissue. These factors are listed in Table 2.
Table 2.
Factors affecting the optical properties of natural teeth and tooth-coloured restorative materials.
Light quality Tooth surface texture and gloss Composition and structure of the substrate (enamel, dentine or restorative material) Thickness of the substrate Translucency or opacity Opalescence, fluorescence or iridescence Characterisations and intensive colours
Light quality
Light quality is highly influential on tooth shade determination. The colour temperature of a light source is measured by the unit degrees kelvin (K). The international standard (ISO) for colour matching is 5500K, which encompasses the full spectrum of colour wavelengths. Repetition of colour assessment under different light sources is also recommended to avoid metamerism, a phenomenon whereby colours can appear substantially different under varying lighting conditions (Figure 5).
Figure 5.
The effect of different colour temperatures of the light sources on the same clinical view. (a) Daylight 5200k; (b) automatic white balance; (c) Shade 7000K; (d) cloudy 6000K; (e) white fluorescent 4000K; (f) tungsten 3200K; (g) flash.
Daylight quality undergoes tremendous variation throughout the day (from 1000K to 20,000K), and the lights on the dental unit and in the operatory can have large variations in the wavelengths of emitted light. An artist will attest that the purest light is the northern light at noon, which should be used whenever possible. There is some truth in this, with many clinicians taking the patient to a window to use natural light to shade match. Unfortunately, it is not practical to have every patient booked in for a 12 noon appointment. It is, therefore, recommended to install daylight corrected bulbs in the surgery and consider using specialised hand-held, colour-corrected light sources for colour matching in dentistry.
While bright illumination is essential for perceiving subtle variations in hue and chroma, lower intensity light may be used for studying value. This also allows enhanced perception of surface texture detail.
Tooth surface texture and gloss
The topography of the surface of the tooth, namely macro- and micro-surface texture and surface gloss features, greatly influences the way that natural teeth interact with light. These are set out in Table 3 and illustrated in Figure 6.
Table 3.
Surface texture features that influence the way that natural teeth interact with light.
Surface texture anatomy increases the value (brightness) of teeth as seen in these maxillary central incisor teeth.
Composition and structure of the substrate (enamel, dentine or restorative material)
The ‘natural layering concept’ was postulated by Didier Dietschi in a series of papers published in the late 1990s and early 2000s.1,2,3,4 Instead of measuring the optical characteristics of teeth as a single unit, the properties of natural dentine and enamel were measured separately. It was found that the variation in the value and hue of dentine was not significantly different between groups of teeth, but what differed was the level of saturation, or chroma.
Apropos of this work, a resin-based composite system was developed to restore missing dental hard tissue using differing shades, opacities and translucencies to match fluorescence and opalescence, similar to natural tissues. Furthermore, the ‘natural layering concept’ also recognised the changes that occur over the life of a tooth regarding its optical properties and structure. Young teeth are whiter by dint of their lower mineral content. They possess a lower dentine chroma and usually have a highly opalescent enamel, whereas adult teeth have a more saturated dentine and a more neutral enamel. Older teeth are darker owing to a continuous increase of dentine chroma as mineralisation increases, and there is deposition of secondary and tertiary dentine along with a more translucent and thinner enamel, which gives a greyish appearance. As a result, the underlying dentine becomes more visible, or even exposed in the case of non-carious tooth surface loss. Furthermore, extrinsic and intrinsic stains may be evident, also influencing the shade of the tooth. Figure 7 shows the difference in appearance between incisors in a younger and older patient.
Figure 7.
Two clinical photographs demonstrating the difference between (a) a younger incisor tooth, and (b) one that has been in the mouth for a number of decades.
Thickness of the substrate
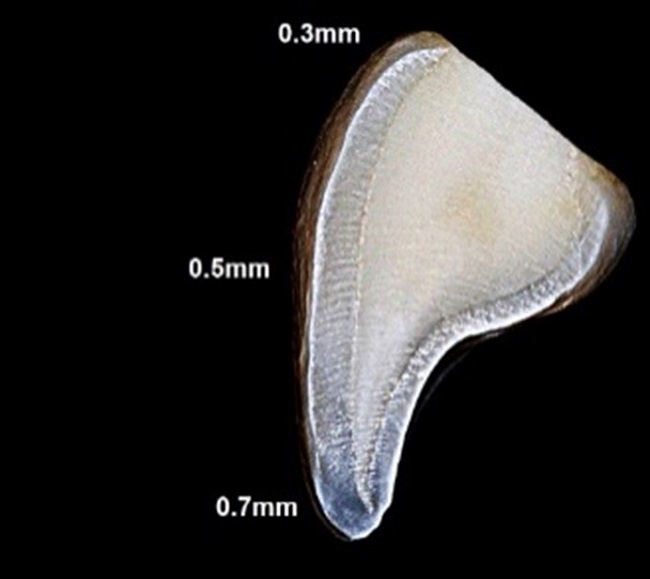
The thickness of the substrate will determine its optical properties. For example, enamel is important in altering the perception of tooth colour and its thickness varies depending on its position in the tooth and the type of tooth (Figure 8).
Figure 8.
The average enamel thicknesses as demonstrated on the labial surface of a maxillary incisor tooth.
Typically, the thicker the enamel present, which is often seen in younger patients, the higher the visual value. As the patient ages, the enamel thickness reduces as a result of pathological or physiological tooth wear processes. The combination of reduced enamel thickness and loss of surface morphology and texture allows for light to be more easily transmitted through the tooth. This in turn makes the teeth appear more translucent and lower in value.
Translucency or opacity
Translucency is regarded as one of the most important factors influencing aesthetics because it determines how much of the underlying dentine, deeper restorative material layers and dark background of the oral cavity show through. One of the most difficult tasks in dentistry is to define the degree of enamel translucency, and for this reason many layering resin-based composite systems are available, in a range of shades, offering different translucencies (Figure 9).
Figure 9.
Note the differing degree of enamel translucency in these incisor teeth. In order to provide an imperceptible restoration in resin-based composite for example, the product must contain a range of shades offering different translucencies.
Generally, the translucency of resin composite is related to its thickness and dimensions, and the proportions of dentine and enamel layers greatly influence the final outcome of a layered composite restoration. There is also a high correlation between translucency and value, with lighter shades having greater translucency. The clinician should therefore pay close attention to the correct layer thicknesses when using a layering resin-based composite system.
Natural teeth have unique, complex, colour variations that are perceived and interpreted by the human brain. In some clinical situations, imperceptible integration of resin-based composite restorations cannot be achieved without sophisticated blending of colours, by the placement of multiple layers with different optical properties.5 The more translucent incisal shades of a layering resin-based composite material (Figure 9) allow the precise replication of complex optical properties caused by localised anatomical variations, such as those listed below and illustrated in Figure 10.
a
b
c
d
Figure 10.
(a–d) Demonstrating the phenomena of opalescence, fluorescence or iridescence, characterisations and intensive colours as described in the text.
Opalescence, fluorescence or iridescence, characterisations and intensive colours
The above terms are defined below:
Opalescence is the property of a translucent material to reflect and transmit the blue and orange-yellow waves of natural light. Hydroxyapatite crystals in enamel act like prisms, giving teeth a blue or amber appearance under transmitted and reflected light, respectively (Figure 10a, b).
Fluorescence is the absorption of light, primarily by the dentine, causing spontaneous emission of a brighter, longer wavelength of light.
Iridescence describes the phenomenon that as the angle or view or illumination changes, so the surfaces of certain substances appear to change colour gradually. This is due to the interference of light waves in thin films or microstructures.
Halo effect is the phenomenon that occurs where aprismatic incisal edge enamel lies adjacent to translucent, highly organised, densely-packed hydroxyapatite crystals (Figure 10b) causing the appearance of a halo in the enamel.
Characterisations are localised, mineralisation differences of varying aetiologies that are common in tooth structure. They may result in a range of white patches and unusual colourations (Figure 10c).
Intensive colours are white or coloured areas of differential mineralisation, and are variations of abnormal anatomy (Figure 10d).
Clinical application of shade selection
Digital
Specialised colour-measuring instruments, termed spectrophotometers, are available to assist in shade matching in dentistry. It is important to note that these devices require fixed lighting and observer conditions, and they are designed to measure flat surfaces, which complicates viewing geometry, such as for curved surfaces. They are prone to significant ‘edge loss’ and are expensive to purchase. Owing to these shortcomings, shade determination is commonly performed visually using commercially available shade guides (Figure 4). However, commercially available shade guides also have a significant shortcoming. The material from which the tabs is fabricated is not the same material to which the shade is being matched, which makes exact shade matching almost impossible. In order to overcome this, the use of custom-made shade guides has been advocated.6
General principles for shade matching using a conventional shade guide technique
To distil and summarise the foregoing, the following recommendations should be followed when shade matching in a dental clinic.
Tooth shade should be measured in daylight, not under artificial lights, and ideally using colour-corrected light sources.
Shade taking should be carried out as soon as possible because teeth rapidly dehydrate and can lighten by one full shade in less than 3 minutes.5
An observation distance of approximately 25 cm is recommended to optimise visual acuity and ocular convergence angle.
Multiple angles of view should be employed.
Value should also be assessed from further away (e.g. 1 metre), and when squinting.
Bright colours should be avoided in the surrounding environment, for example lipstick, clothing and surgery decor.
Shade should be taken within 5–7 seconds because cones in the retina rapidly accommodate to similar yellow and red colours.
When shade taking, the first impression is usually the most accurate.
Blue backgrounds are sometimes suggested to rest and re-accommodate cones to the spectrum of tooth colours, but this may cause after-images or bias colour perception.
A team approach to shade taking is recommended to minimise personal variables.
Traditionally, females were considered to be more accurate at shade selection; however, it is now believed that there is no significant sexual dimorphism.7,8,9,10
Colour ‘blindness’ and shade taking
The condition colour ‘blindness’ or colour vision deficiency (CVD) is a congenital condition affecting both eyes. It affects more males (one in 10) than females (one in 200) and is not fully understood. The retinal cones are not as sensitive with an inability to register red, green and blue colours, meaning that the colours look similar. The ramifications for shade determination in dentistry for affected individuals is that errors in hue and chroma can occur, but value is not affected.
Conclusion
Colour matching is an essential skill in dentistry and has been demonstrated to be significantly improved by education and training programmes. The present article has outlined the physics behind the art of shade determination, and has illustrated how this underpins the clinical procedure. The next article in the series will deal with shade matching when using a resin-based composite material directly, and the third will consider indirect restorations featuring fundamental, intermediate and advanced shade-matching tips designed to help clinicians increase the quality, consistency, speed and predictability of shade-matching procedures.