Comba A, Vergano EA, Baldi A 5-year retrospective evaluation of direct composite restorations in orthodontically treated patients. J Dent. 2021; 104 https://doi.org/10.1016/j.jdent.2020.103510
Garcia-Torres F, Jurado CA, Rojas-Rueda S Combining orthodontic and restorative care with novel workflows. Dent J (Basel). 2024; 12 https://doi.org/10.3390/dj12070218
Schneider UEM, Moser L Achieving excellence with interdisciplinary approaches in complex orthodontic adult patients. Br Dent J. 2024; 237:349-359 https://doi.org/10.1038/s41415-024-7778-9
Sousa J, Azevêdo AB, Santos R Survival of teeth with external cervical resorption after internal and external repair: a systematic review. J Clin Exp Dent. 2024; 16:e1555-e1563 https://doi.org/10.4317/jced.62050
Interdisciplinary collaboration is essential for managing complex dental cases, ensuring predictable outcomes and patient satisfaction. This case report describes the comprehensive treatment of a patient with severe dental wear, requiring a combination of orthodontic and restorative interventions. The initial treatment plan included orthodontic correction to create space for restorative work. However, unforeseen challenges, such as short clinical crowns and deep bite-related bracket debonding, required an adjustment in the treatment sequence. Early restorative intervention with direct composite build-ups enabled successful orthodontic progress. The final phase included definitive composite restorations and retention to ensure occlusal stability and to help the patient smile again. This case emphasizes the importance of timely coordination among specialists, shared decision-making and adaptability in treatment planning. The patient reported high satisfaction with both aesthetic and functional outcomes. This case highlights the value of interdisciplinary collaboration in achieving optimal, long-term dental rehabilitation results.
CPD/Clinical Relevance: Collaboration with other disciplines, timely coordination and regular consultations ensure a win–win situation.
Article
Interdisciplinary collaboration is essential for effectively managing complex dental cases, especially for patients with severe tooth wear and a need for orthodontic treatment. Coordinated efforts among orthodontists, restorative dentists and endodontists ensure that both functional and aesthetic rehabilitation is predictable and durable.1 Integrating orthodontic treatment with restorative dentistry facilitates space creation, bite correction and optimal tooth positioning prior to placing final restorations.2,3 Nonetheless, challenges, such as deep bites, short clinical crowns and bracket debonding, may require adjustments to the initial treatment sequence to secure successful outcomes.4
This article presents a case of severe dental wear managed through a staged orthodontic and restorative approach. Early complications necessitated mid-treatment composite restorations to stabilize the occlusion before further orthodontic progress could continue. The case highlights the importance of communication and shared decision-making among dental specialists, ultimately resulting in a well-functioning, aesthetically pleasing result.
Effective communication before initiating treatment is essential to ensure a well-coordinated, predictable and successful outcome. Clear interdisciplinary planning helps identify potential challenges, align treatment goals and optimize patient care, ultimately preventing complications and ensuring long-term stability. Therefore, this case report provides insights into best practices for interdisciplinary treatment planning in complex dental rehabilitation cases.
Referral to the orthodontist
A 54-year-old male patient presented for an initial consultation, seeking restoration of his severely worn teeth, which were causing both functional and aesthetic concerns (Figure 1). His own dental practitioner had referred him with the expectation of a prolonged orthodontic treatment, potentially combined with orthognathic surgery.
Figure 1.
(a–c) Pre-treatment extra-oral views.
A clinical examination revealed a neutral skeletal relationship, a harmonious facial profile, neutral occlusion and a deep bite. The dental arches were well aligned, and there was significant wear on the upper and lower anterior teeth, as well as on LL7 and LR7. The occlusion was stable, and the masseter muscles were pronounced bilaterally. His oral hygiene was excellent, with only a few restorations. UR3 and UL6 had undergone endodontic treatment, with the UR3 showing an apical radiolucency, although it was asymptomatic. UL6 was restored with a crown (Figure 2).
Figure 2.
(a–f) Pre-treatment intra-oral views.
Complexities of the case
The primary complicating factors included:
Aesthetic and functional concerns;
Deep bite with uneven occlusal curves;
Localized severe wear (teeth LL7, LR7, and anterior segments in upper and lower jaw);
Apical pathology on tooth UR3.
The patient expressed disappointment that his dentist had never addressed his dental wear or the complexity of his case. He had numerous concerns and questions regarding his condition and sought clarification on why no prior intervention had been suggested. After reassurance, emphasizing that his condition was a dental rather than a skeletal problem, orthodontic treatment was deemed essential as an initial phase to facilitate subsequent restorative procedures.
Initial treatment plan
The proposed treatment plan included:
Explanation of the treatment approach and consultation with a restorative specialist;
Endodontic revision of tooth UR3;
Fabrication of a bite-raising appliance to protect the lower fixed orthodontic appliance;
Placement of fixed appliances on the lower dentition;
Placement of fixed appliances on the upper dentition;
Direct composite restorations for the upper and lower anterior teeth;
Permanent retention using two continuous bonded retainers.
Phase 1: start of treatment
The orthodontic treatment aimed to correct occlusal curves, eliminate the deep bite, and create space for the restorative phase. Once the orthodontic treatment had been completed, the restorative phase would take place by rebuilding the upper and lower anterior teeth with direct composite restorations to enhance aesthetics. To ensure seamless integration of the restorative phase with the orthodontic treatment, the treatment plan was discussed and coordinated with a restorative dentist to determine the optimal timing for the restorative procedure. The patient agreed to the proposed treatment plan.
Before orthodontic treatment, an endodontist re-treated UR3 and diagnosed a cervical external inflammatory resorption process.5 The defect became visible after cleaning the pulp chamber and root canal, and was located disto-palatally to the pulp chamber, below the cemento-enamel junction. She cleaned the defect from the inside, and filled it with mineral trioxide aggregate (MTA), but was unsure whether all the resorptive tissue had been completely removed. The uncertain condition of the tooth was discussed with the patient. He opted to keep the tooth for as long as possible, knowing that extraction could always be considered later if necessary, and that future implant placement remained a potential option. Furthermore, leaving the tooth in situ would be advantageous during orthodontic treatment (e.g. for preservation of bone height and volume).
Phase 2: emerging challenges
An orthodontic appliance was prescribed to raise the bite as the as the initial step in orthodontic treatment. It was intentionally selected to begin the treatment process with this method. Although this adaptation phase can often be challenging for many patients, successful acclimatization enabled the safe placement of the lower brackets (LL7–LR7) without the risk of fracture. However, owing to the short clinical crowns of the lower incisors, achieving bracket adhesion was difficult and the patient experienced frequent debonding of the brackets on the lower anterior teeth. Furthermore, the patient experienced difficulties with adaptation to the bite-raising appliance. It soon became clear that the treatment would not be as straightforward as initially anticipated, and issues emerged that could not easily be solved. To overcome this impasse, the restorative dentist was consulted sooner than expected. It was discussed how the orthodontic treatment could be continued, ensuring that the brackets could better adhere to the lower anterior teeth. A modified approach was decided, which involved preliminary restorative intervention before continuing orthodontic treatment. The solution was to start to restoratively build-up the lower anterior teeth LL3–LR3 in an increased vertical dimension of occlusion and restore the anatomical shape of LL7 and LR7.
Phase 2a: modifying the restorative approach
The orthodontic treatment was temporarily interrupted 3 months after it began and the brackets on teeth LL3–LR3 were removed. The anterior lower teeth were restored with freehand direct composite restorations (Filtek Supreme XTE, shade A2B, 3M), anatomically rebuilt at an increased vertical dimension. The prescribed increase of vertical dimension of occlusion created space, allowing the worn LL7 and LR7 to be anatomically restored with direct composite restorations (Filtek Supreme XTE, shade A2B). The amalgam restoration in LR7 was replaced. To further open the bite and relieve pressure on the anterior teeth, two temporary dorsal stops of resin composite were placed on the premolars. With the restorations now in place, the brackets were re-attached, and the orthodontic treatment continued (Figure 3).
Figure 3.
(a–f) Phase 2a orthodontic treatment.
Phase 3: continuation of orthodontic treatment
After the restorative treatment of the lower anterior teeth, fixed orthodontic appliances were placed in the upper jaw from UR7 to UL7, and on the restored lower anterior segment. The orthodontic treatment then progressed smoothly, with no further debonding of the brackets. The treatment continued systematically, following a sequence of archwires (lower jaw: 018 NiTi, 18x18 NiTi, 18x25 NiTi, 17x25 stainless steel; upper jaw: 16x16 NiTi, 18x18 NiTi, 18x25 NiTi, 16x22 stainless steel). The patient maintained good oral hygiene and remained motivated to complete the treatment plan.
One year after the start of phase 3, a new consultation took place with the restorative dentist to discuss any necessary adjustments before debonding and reconstructing the remaining teeth (Figure 4). The restorative dentist wished to intrude tooth UR3 by an additional 2 mm to create sufficient space for the restorations. Tooth UL3 was already in the correct position, and the achieved horizontal open bite in the anterior region was satisfactory.
Figure 4.
(a–f) One year after treatment initiated.
Phase 4: restorative treatment
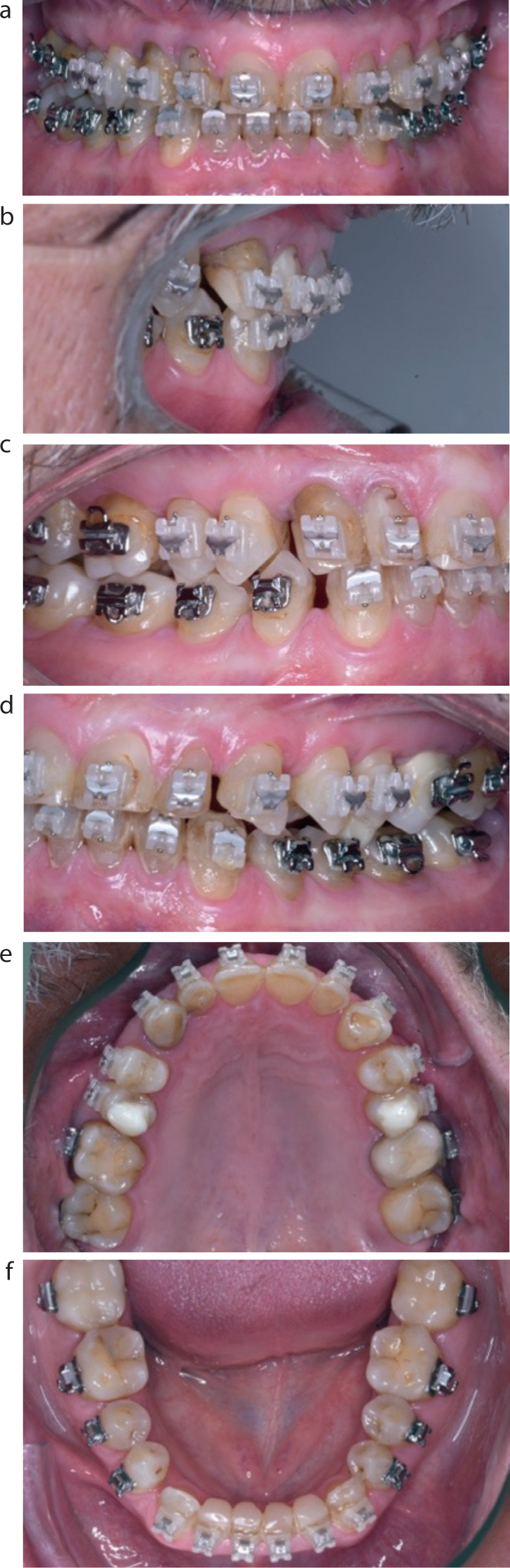
The final orthodontic adjustments were completed 2 years after the start of treatment (Figure 5). The appointment for debonding the orthodontic appliances was coordinated with the restorative treatment. At this point, no permanent retention had been placed to allow for the restorative procedures to be carried out, and which would need to be finished as soon as possible to minimize the risk of relapse.
Figure 5.
(a–i) Post-orthodontic debond.
During the first restorative appointment, the upper anterior teeth (UR3–UL3) were built up using freehand direct composite restorations (Filtek Supreme XTE, shade A2B). To ensure adequate volume and strength, the palatal surfaces were thickened, and all teeth were lengthened according to a previously made intra-oral mock-up (‘lip generated smile design’).6 In the same session, direct composite veneer restorations were placed on the upper anterior teeth (Filtek Supreme XTE, shade A2B). This restorative treatment enhanced aesthetics and restored the occlusal curve. Finally, the temporarily built-up lower incisors were replaced and adjusted to the new situation. After the restorative treatment, permanent retention wires were placed behind both the upper and lower anterior teeth to prevent any relapse.
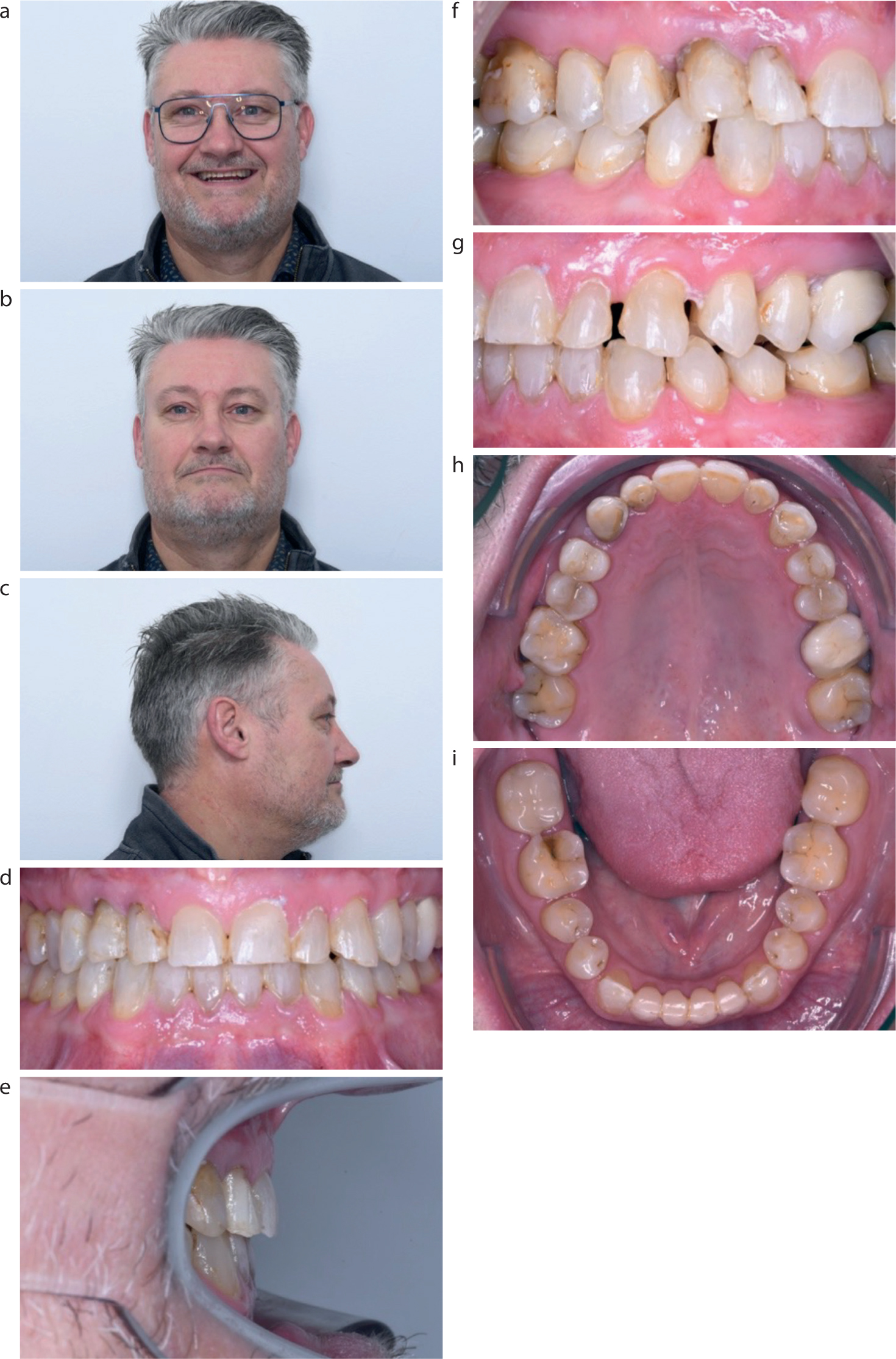
The patient's reaction was extraordinary. He understood that the entire process was complex and that a well-structured ‘construction plan’ was essential. He appreciated the interdisciplinary discussions and felt supported throughout the process. At the first recall after the restorations were completed, his eyes sparkled with joy, and he was excited about the result. He was extremely satisfied with the outcome and enjoyed his new appearance and better smile. He felt 10 years younger and good function had been restored to his teeth (Figure 6).
Figure 6.
(a–i) Post final restorative treatment.
Patient experience and reflection
The treatment took 2 years, during which time the patient was seen by an endodontist, an orthodontist and a restorative dentist. The primary goal of the treatment was to restore the aesthetics caused by tooth wear due to the unfavourable orthodontic relationship and extreme frontal deep bite. In retrospect, we can confidently say that this goal was achieved. The patient is highly satisfied with the aesthetically pleasing and well-functioning result.
Unfortunately, the initial treatment plan had to be modified once the orthodontic treatment had already begun. This modification and adjustment to the planned sequence of phases were necessitated by the small size of the lower anterior teeth and the deep bite. The brackets did not stay in place on the lower anterior teeth, making it essential to restore the lower incisors before continuing with the orthodontic treatment. This change in the treatment plan ensured that the orthodontic phase progressed smoothly, ultimately leading to a successful outcome and patient satisfaction.
Tooth UR3 was diagnosed with cervical external root resorption prior to the start of orthodontic treatment and was deemed to have a moderate to poor prognosis. During a consultation with the patient, which involved shared decision-making, it was decided to retain this tooth for as long as possible while integrating it into the overall treatment plan. Although this is not an optimal situation, the patient was fully informed and understood that if complications arose with this tooth, it might be lost and alternative options, such as an implant, can still be considered. Extracting and placing an implant before completing the orthodontic treatment would have resulted in an unfavourable situation and significant loss of alveolar bone height. Now that the orthodontic treatment is complete, the teeth are aligned and restored, making the replacement of this tooth with an implant much more predictable. However, 2 years after the end of the treatment, UR3 was still in place.
Reflecting on the situation, we believe that further intrusion of the lower anterior teeth could have enhanced the final outcome. Intrusion is a complex and time-consuming process that requires careful planning and patient cooperation. Additionally, patients often become satisfied with the aesthetics of their teeth early in treatment and may grow impatient with continued orthodontic adjustments. Another factor that may have contributed to the residual deep bite was the orthodontist's underestimation of the amount of composite material needed for the restorations. The intrusion of the lower anterior teeth might have helped achieve a more stable and functionally optimal result.
Collaboration with other disciplines, timely coordination of treatment plans and regular intermediate consultations ensured that a true win–win situation was achieved in this complex case. A patient who experiences this mutual coordination and professional respect thrives in such teamwork. Communication was efficient and agreements were clear. Therefore, we can say that this was a true win–win–win situation, benefiting the patient and both treating clinicians. Now that's what we call great teamwork!
Conclusion
Collaboratively managing a clinical case is significantly more effective and fulfilling than working in isolation. However, many clinicians hesitate to seek advice from their colleagues. It is crucial to acknowledge that no single practitioner can possess comprehensive expertise in all areas. Seeking guidance and establishing a treatment plan from the outset can facilitate an efficient and cohesive workflow. Using digital tools for communication, email consultations and planning enhances interdisciplinary collaboration, ultimately benefiting the patient.