Ponnusamy S, Gonzalez J, Holtzclaw D A systematic approach to restoring full arch length with maxillary fixed implant reconstruction: the PATZi protocol. Int J Oral Maxillofac Implants. 2023; 38:996-1004 https://doi.org/10.11607/jomi.10153
Araujo RZ, Santiago Júnior JF Clinical outcomes of pterygoid implants: systematic review and meta-analysis. J Craniomaxillofac Surg. 2019; 47:651-660 https://doi.org/10.1016/j.jcms.2019.01.030
Balshi TJ, Wolfinger GJ, Slauch RW, Balshi SF Brånemark system implant lengths in the pterygomaxillary region: a retrospective comparison. Implant Dent. 2013; 22:610-612 https://doi.org/10.1097/ID.0b013e3182a5d181
Stefanelli LV, Graziani U, Pranno N Accuracy of dynamic navigation surgery in the placement of pterygoid implants. Int J Periodontics Restorative Dent. 2020; 40:825-834 https://doi.org/10.11607/prd.4605
Rasaie V, Abduo J, Falahchai M Clinical and laboratory outcomes of angled screw channel implant prostheses: a systematic review. Eur J Dent. 2022; 16:488-499 https://doi.org/10.1055/s-0041-1740298
Su H, Gonzalez-Martin O, Weisgold A, Lee E Considerations of implant abutment and crown contour: critical contour and subcritical contour. Int J Periodontics Restorative Dent. 2010; 30:335-343
Dynamic navigation and intra-oral photogrammetry for the immediate full-arch rehabilitation of a severely resorbed maxilla: a case report Aly Virani Aesthetic Update 2025 2:1, 41-44.
Authors
AlyVirani
BDS (Hons), Dip MJDF(RCSEng), Assoc FCGDent, Dip Imp Dent RCSEd, MSc (Clinical Oral Implantology), Implant Dentist and Clinical Director, North Cardiff Dental and Implants, Cardiff, Wales
A 69-year-old female patient with osteoporosis and severely resorbed maxilla presented with unrestorable caries, porcelain fracture, and multiple apical infections on the root-treated abutments of a 10-unit maxillary bridge. The treatment plan comprised bilateral pterygoid implants, incisive canal placement of a wide-diameter implant, and bilaterial tilted implants. The surgery was planned to use Navident EVO dynamic navigation system. Accurate placement of all implants was achieved, including the technique-sensitive pterygoids. High primary stability enabled immediate loading, with photogrammetry used to produce a provisional prosthesis. All implants integrated successfully, with the final restoration fitted 4 months post-surgery.
CPD/Clinical Relevance: This is the first documented use of dynamic navigation computer aided dental surgery to facilitate the accurate placement of pterygoid implants in the UK to enable immediate full arch rehabilitation of the severely atrophic maxilla.
Article
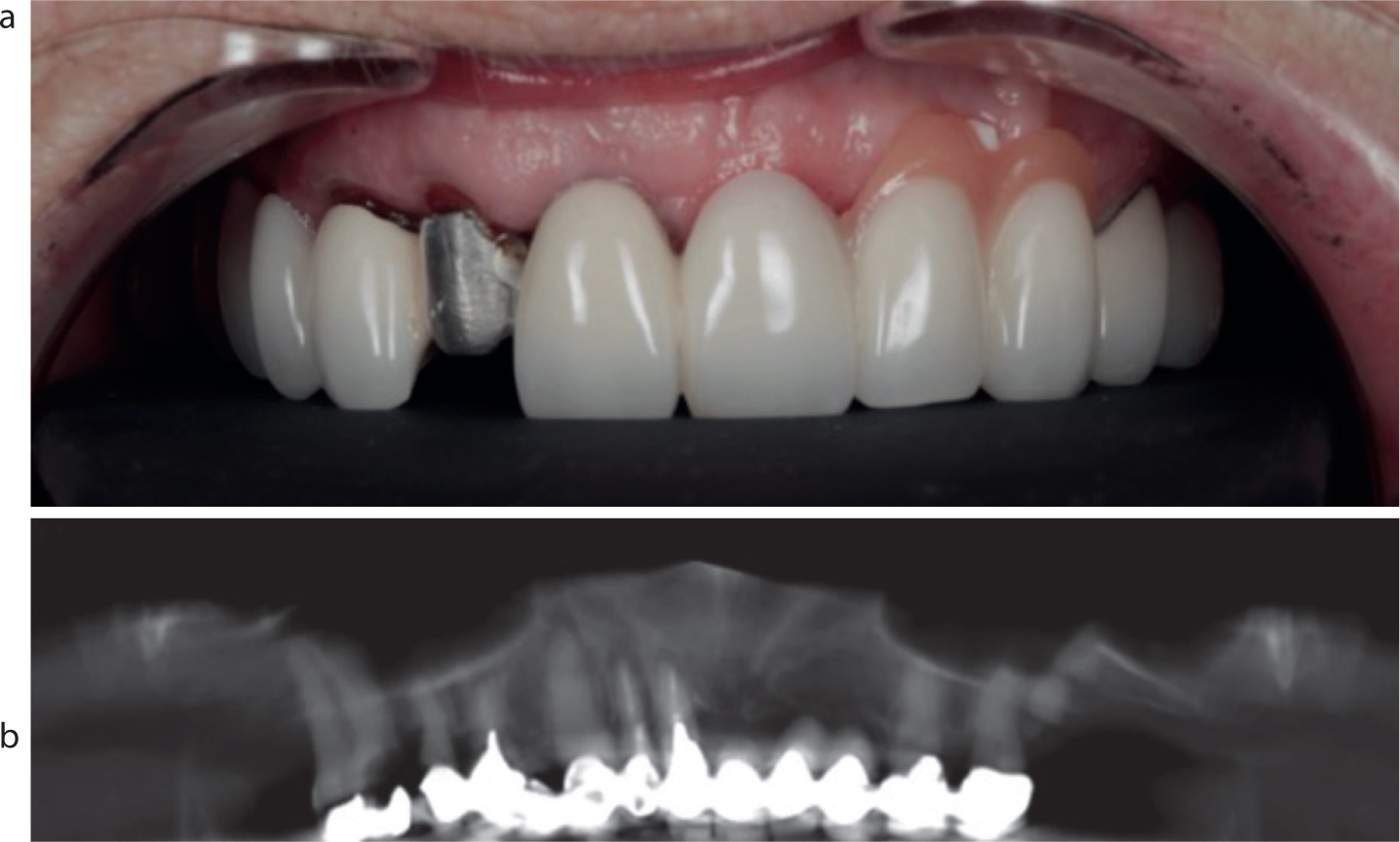
A 69-year-old female patient with osteoporosis presented with unrestorable caries (UR6), porcelain fracture, and multiple apical infections on root-treated abutments of a 10-unit maxillary bridge. Clinical assessment of the CBCT revealed pneumatized sinuses as well as limited bone width in zone 1 and no bone in zones 2 and 3 (Figure 1). As such, the following treatment plan was formulated using the PATZi protocol:1
Bilateral pterygoid placement (Southern Implants, Irene, RSA) 4.0 mm diameter, 15 mm length, deep conical connection);
Incisive canal placement of a wide-diameter implant (Southern Implants, 6.0 mm diameter, 10 mm length, external hex connection);
Bilateral placement of tilted Co-Axis implants (Southern Implants 4.0 mm diameter, 15 mm length, 24° external hex connection);
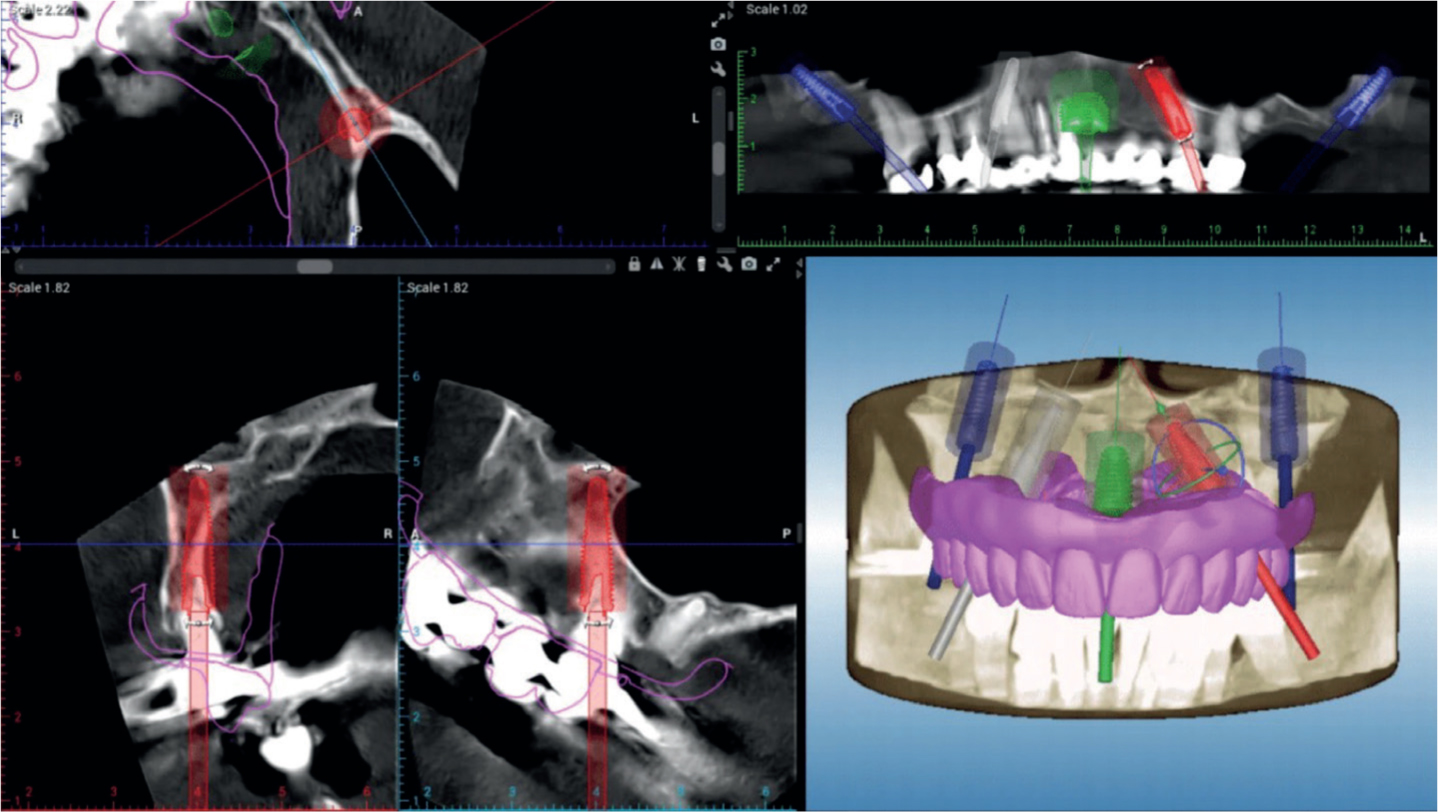
The implant position was planned using Navident software, combined with the digital wax-up to ensure feasibility (Figure 2). This was sent to the laboratory for fabricatation of a prosthetic envelope and bone reduction guide.
The surgery was planned to be performed using real-time visual guidance (Navident EVO, ClaroNav Dental, Ontario, Canada).
Figure 1. Initial presentation of the patient showing the caries, apical radiolucencies, and pneumatized sinuses.Figure 2. Combined digital wax-up and implant positioning plan.
On the day of surgery, screws (Ustomed, Tuttlingen, Germany) were placed in the palate to act as a tracing point for the Navident dynamic navigation, as well as to provide a reference point for the laboratory. An ultra-low dose pre-operative CBCT was taken to capture the screw position digitally. The Navident tracer and jaw trackers were then used to register the patient's'anatomy. This digital file was then compared to the pre-operative CBCT to confirm a registered accuracy of 0.1 mm.
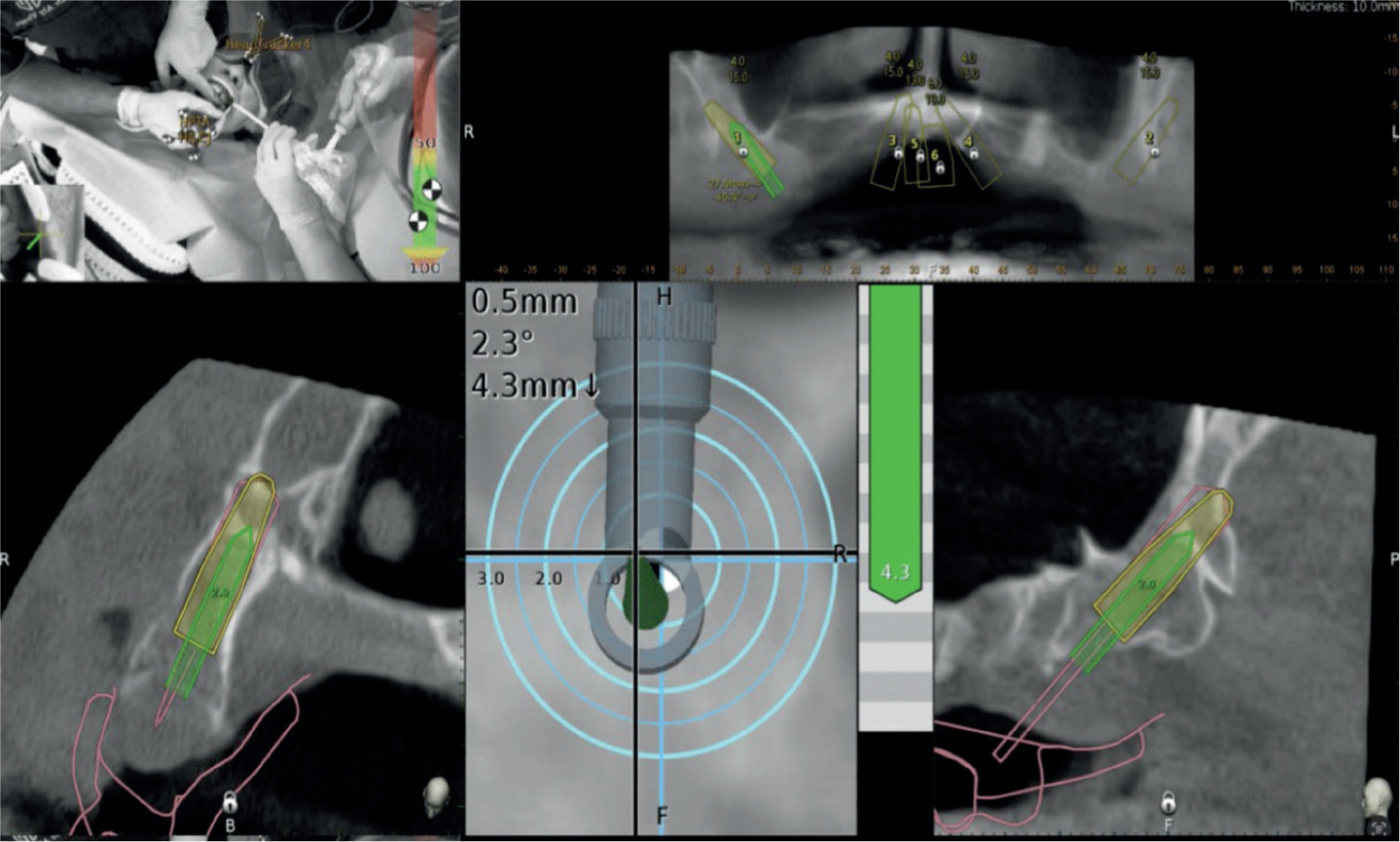
A flap was raised and osteotomy preparation for the pterygoid implants conducted first as per the PATZi protocol.1 A W&H handpiece was fitted with a Navident Handpiece Tracker and the system used to project the planned site location onto the patient. The manufacturer's drilling protocol was followed, which involves the use of a single drill (D-3SPADE-1.8M). The 3D position of the drill can be visualized in real-time on the Navident display to facilitate osteotomy depth and angulation in line with the preplanned implant position (Figure 3). The right and left pterygoid implants were then placed by hand. Over 50 Ncm of torque was achieved on both implants, and the 30° multi-unit abutments (MUAs) were connected (Figure 4).
Figure 3. Real-time visualization of UR pterygoid osteometry preparation to guide angulation and depth according to the planned implant position.Figure 4. 30° multi-unit abutment connected to UL pterygoid implant.
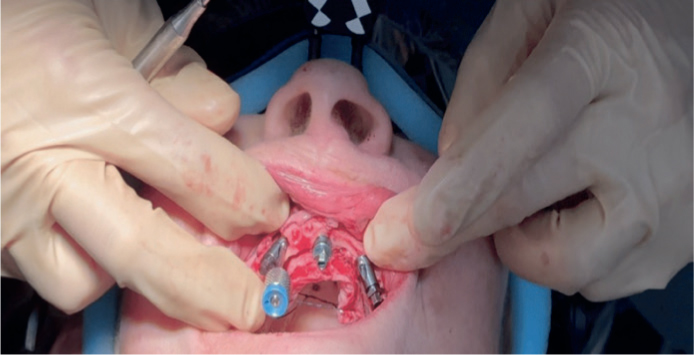
The patient's bridge was removed in one piece and individual extraction of the remaining tooth roots performed. The prefabricated guide was used for ridge reduction. The manufacturer's drilling protocol was followed in conjunction with the Navident system to drill the UL osteotomy. A palatal approach was required owing to limited bone width. Drilling of the nasopalatine and UR site was conducted in a similar manner, and the implants placed. Over 50 Ncm insertion torque and 120 Ncm composite torque value (CTV) was achieved across all implants. Southern Implants straight MUAs with a built-in platform switch were connected (Figure 5).
Figure 5. Positioning of anterior implants including the built-in angle correction of the bilaterial Co-Axis implants.
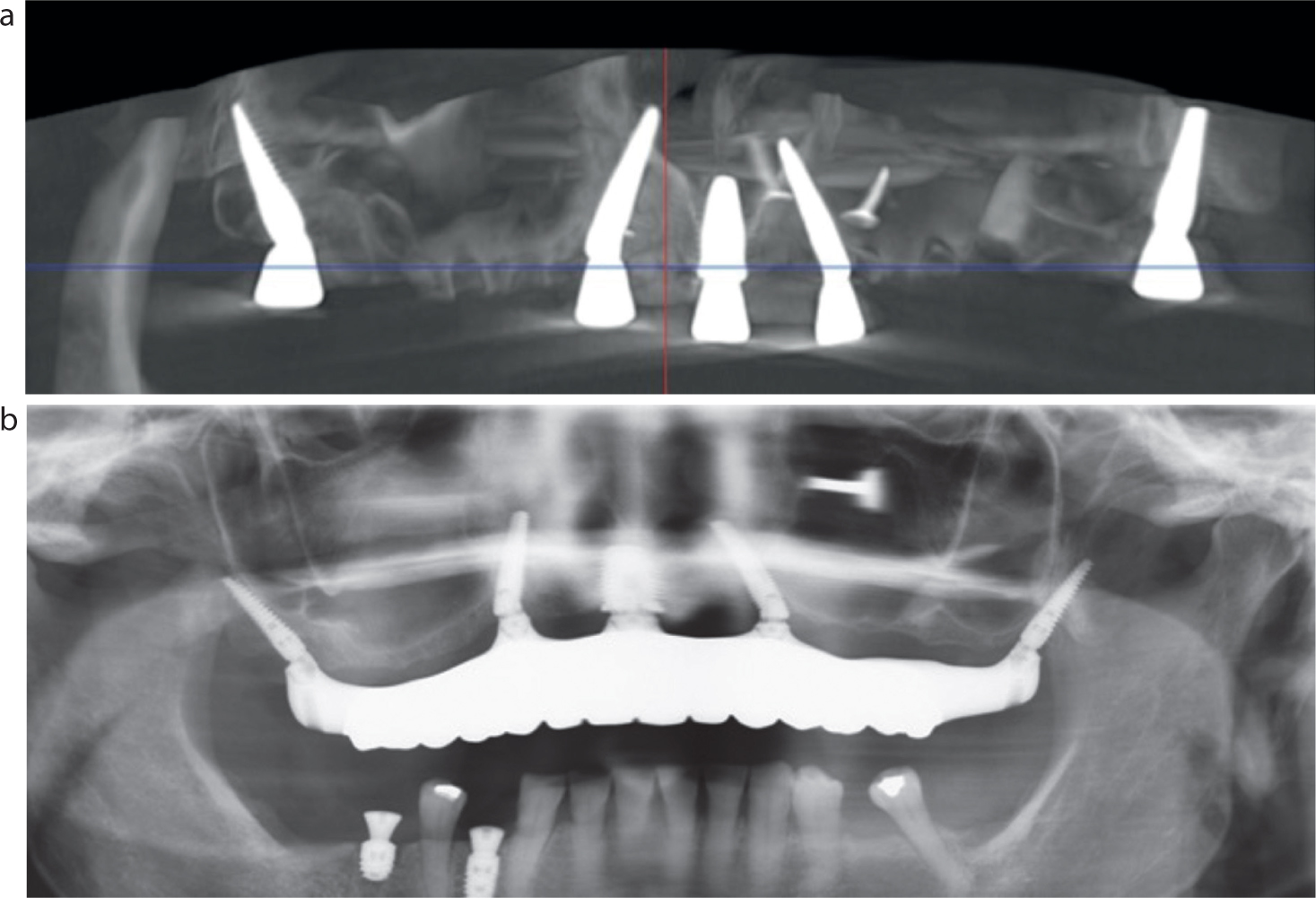
The flap was closed and a post-operative intra-oral scan taken to capture the soft tissue profile. Photogrammetry scans (Aoral Elite, Shining 3D, Hangzhou, China) were then taken to capture the implant positions as well as an ultra low-dose CBCT. These digital files were merged with the digital wax up to fabricate a direct-to-MUA temporary prosthetic design with oral hygiene channels. This prosthesis was 3D printed in SprintRay Crown (SprintRay EU, Weiterstadt, Germany) for next day fit (Figure 6).
Figure 6. Post-operative CBCT showing engagement of pterygoid plates in the posterior as well as radiograph demonstrating ability of photogrammetry to produce an accurate fitting restoration.
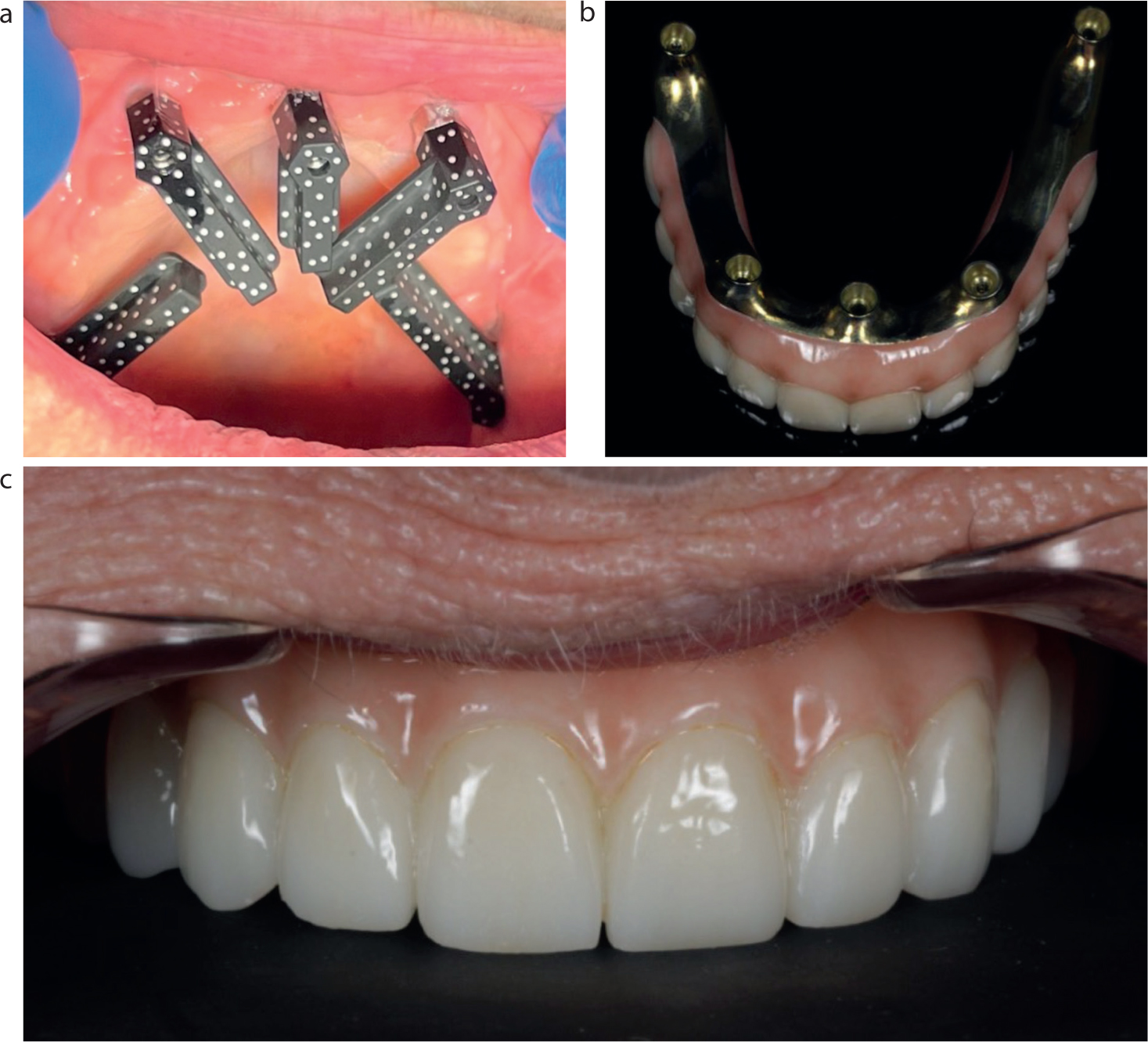
Following an uneventful 4-month healing period, integration of the implants was confirmed and intra-oral photogrammetry used to record the implant positions before a final restoration was constructed using a titanium bar with an overlaying zirconia sleeve (Figure 7).
Figure 7.
(a) Intra-oral photogrammetry; (b) final prosthesis; and (c) final restoration in situ.
Discussion
The PATZi (pterygoid, anterior, tilted, zygomatic, implants) protocol was developed for planning and performing full-arch implant treatments in patients with severely atrophic maxillae. It allows a surgeon to appropriately sequence the use of complex techniques to facilitate improved composite torque value, antero-posterior (AP) spread, and eliminate distal cantilever forces without the additional time and costs associated with grafting procedures.1
The patient's anatomy facilitated the use of bilateral pterygoids in line with the ‘P’ from PATZi. The placement of pterygoid implants requires accurate implant insertion and positioning to cross the maxillary tuberosity area and engage the dense pterygomaxillary plate. Several studies acknowledge that a learning curve is required to achieve accurate placement.2
Computer-aided design/computer-assisted manufacture (CAD/CAM) enables prosthetically driven surgical templates to be fabricated and used to pinpoint placement of pterygoid implants into the dense cortical bone, with Balshi et al finding no statistical difference in cumulative survival rates of immediately loaded pterygoid implants when placed freehand or guided (NobelGuide or NobelClinician stereolithic surgical template, Nobel Biocare Services AG, Zürich-Flughafen, Switzerland).3
This case report shows that dynamic navigation provides another potential option to achieve accurate pterygoid implant placement.4 Furthermore, dynamic navigation combined with the single-drill protocol and self-tapping threads of the Southern Implants pterygoid implant allowed for a highly efficient workflow, high primary stability, and favourable emergence.
Following pterygoid placement, the ‘A’ and ‘T’ of the PATZi protocol were satisfied, with the Co-Axis subcrestal angle correction feature from Southern Implants selected as the ‘tilted’ implants to engage the limited bone while maintaining favourable screw access through the cingulum. This enabled straight MUAs to be fitted to the tilted implants, which requires less restorative space, promotes stable soft tissue, and decreases the risk of screw-loosening and/or other complications when compared to angled abutments.5,6
The digital workflow precludes the use of the Sheffield test to assess the fit of the final restoration, but a single screw, screw passivity test, as well as the radiograph confirm passivity. As such, this case report confirms the ability of intra-oral photogrammetry to produce accurately fitting restorations digitally.
Conclusion
Dynamic navigation was used for full-arch rehabilitation of a severely atrophic maxilla, including accurate and efficient placement of bilaterial pterygoid implants. Sufficient primary stability was achieved, which enabled immediate loading, and intra-oral photogrammetry facilitated a passive fit of the prosthesis. All implants integrated successfully with the final prosthesis fitted 4 months post-surgery. The patient was highly satisfied with the treatment outcome.