Pham TAV, Nguyen PA Morphological features of smile attractiveness and related factors influence perception and gingival aesthetic parameters. Int Dent J. 2022; 72:67-75 https://doi.org/10.1016/j.identj.2021.02.001
Castro MJ, Mendes JJ, Vinga S, de Andrade DC Differential diagnosis of developmental defects of enamel: a review. Ann Med. 2021; 53:S49-50 https://doi.org/10.1080/07853890.2021.1897305
Gil-Bona A, Karaaslan H, Depalle B Proteomic analyses discern the developmental inclusion of albumin in pig enamel: a new model for human enamel hypomineralization. Int J Mol Sci. 2023; 24 https://doi.org/10.3390/ijms242115577
Bartlett JD Dental enamel development: proteinases and their enamel matrix substrates. ISRN Dent. 2013; 2013 https://doi.org/10.1155/2013/684607
Silva MJ, Scurrah KJ, Craig JM Etiology of molar incisor hypomineralization: a systematic review. Community Dent Oral Epidemiol. 2016; 44:342-353 https://doi.org/10.1111/cdoe.12229
Mahoney EK, Farah R Molar incisor hypomineralization: structure, composition, and properties. Planning and Care for Children and Adolescents with Dental Enamel Defects. 2015; 73-84
Wright JT The etch-bleach-seal technique for managing stained enamel defects in young permanent incisors. Pediatr Dent. 2002; 24:249-252
Santos LFTF, Rêgo HMC, Borges AB Efficacy of bleaching treatment on demineralized enamel treated with resin infiltration technique. World J Dent. 2012; 3:279-283 https://doi.org/10.5005/jp-journals-10015-1173
Marouane O, Douki N, Chtioui F A combined approach for the aesthetic management of stained enamel opacities: external bleaching followed by resin infiltration. Case Rep Dent. 2018; 2018 https://doi.org/10.1155/2018/1605842
Marouane O, Chtioui F Transillumination-aided infiltration: A diagnostic concept for treating enamel opacities. J Esthet Restor Dent. 2020; 32:451-456 https://doi.org/10.1111/jerd.12602
Bozal CB, Kaplan A, Ortolani A Ultrastructure of the surface of dental enamel with molar incisor hypomineralization (MIH) with and without acid etching. Acta Odontol Latinoam. 2015; 28:192-198 https://doi.org/10.1590/s1852-48342015000200016
Bhandari R, Thakur S, Singhal P In vivo comparative evaluation of esthetics after microabrasion and microabrasion followed by casein phosphopeptide-amorphous calcium fluoride phosphate on molar incisor hypomineralization-affected incisors. Contemp Clin Dent. 2019; 10:9-15 https://doi.org/10.4103/ccd.ccd_852_17
Allen DN, Fine CM, Newton MN Resin Infiltration Therapy: A micro-invasive treatment approach for white spot lesions. J Dent Hyg. 2021; 95:31-35
Paris S, Dörfer CE, Meyer-Lueckel H Surface conditioning of natural enamel caries lesions in deciduous teeth in preparation for resin infiltration. J Dent. 2010; 38:65-71 https://doi.org/10.1016/j.jdent.2009.09.001
Subramaniam P, Girish Babu KL, Lakhotia D Evaluation of penetration depth of a commercially available resin infiltrate into artificially created enamel lesions: An in vitro study. J Conserv Dent. 2014; 17:146-149 https://doi.org/10.4103/0972-0707.128054
Arakawa Y, Takahashi Y, Sebata M The effect of acid etching on the cervical region of the buccal surface of the human premolar, with special reference to direct bonding techniques. Am J Orthod. 1979; 76:201-208 https://doi.org/10.1016/0002-9416(79)90121-0
Crombie F, Manton D, Palamara J, Reynolds E Resin infiltration of developmentally hypomineralised enamel. Int J Paediatr Dent. 2014; 24:51-55 https://doi.org/10.1111/ipd.12025
Marouane O, Manton DJ The influence of lesion characteristics on application time of an infiltrate applied to MIH lesions on anterior teeth: an exploratory in vivo pilot study. J Dent. 2021; 115 https://doi.org/10.1016/j.jdent.2021.103814
Kumar H, Palamara JEA, Burrow MF, Manton DJ An investigation into the effect of a resin infiltrant on the micromechanical properties of hypomineralised enamel. Int J Paediatr Dent. 2017; 27:399-411 https://doi.org/10.1111/ipd.12272
Rodrigues MC, Mondelli RF, Oliveira GU Minimal alterations on the enamel surface by micro-abrasion: in vitro roughness and wear assessments. J Appl Oral Sci. 2013; 21:112-117 https://doi.org/10.1590/1678-7757201302117
Amend S, Stork S, Lücker S Influence of different pre-treatments on the resin infiltration depth into enamel of teeth affected by molar-incisor hypomineralization (MIH). Dent Mater. 2024; 40:1015-1024 https://doi.org/10.1016/j.dental.2024.05.010
Akin M, Aksakalli S, Basciftci FA, Demir A The effect of tooth bleaching on the shear bond strength of orthodontic brackets using self-etching primer systems. Eur J Dent. 2013; 7:55-60
Shinohara MS, Peris AR, Pimenta LA, Ambrosano GM Shear bond strength evaluation of composite resin on enamel and dentin after nonvital bleaching. J Esthet Restor Dent. 2005; 17:22-29 https://doi.org/10.1111/j.1708-8240.2005.tb00078.x
Borges AB, Abu Hasna A, Matuda AGN Adhesive systems effect over bond strength of resin-infiltrated and de/remineralized enamel. F1000Res. 2019; 8 https://doi.org/10.12688/f1000research.20523.1
Wiegand A, Stawarczyk B, Kolakovic M Adhesive performance of a caries infiltrant on sound and demineralised enamel. J Dent. 2011; 39:117-121 https://doi.org/10.1016/j.jdent.2010.10.010
Yuan Y, Intajak P, Islam R Effect of sodium hypochlorite on bonding performance of universal adhesives to pulp chamber dentin. J Dent Sci. 2023; 18:1116-1124 https://doi.org/10.1016/j.jds.2022.11.007
Chay PL, Manton DJ, Palamara JE The effect of resin infiltration and oxidative pre-treatment on microshear bond strength of resin composite to hypomineralised enamel. Int J Paediatr Dent. 2014; 24:252-267 https://doi.org/10.1111/ipd.12069
The clinical management of incisor hypomineralisation (IH) as it pertains to biophysical and aesthetic recovery, especially in the teeth of young individuals, is fraught with complexity. Treatment modalities are wide and varied, and often, if used in the wrong sequence, can lead to a suboptimal aesthetic result. Approaches, such as chemical micro-abrasion, air particle abrasion and tooth whitening have been used in the past, in addition to resin infiltration for the treatment of affected enamel. The penetration depth of hypomineralised lesions by resin infiltrant has been reported to vary and be dependent on the pre-treatment modalities used. The elimination of brown-coloured aspects of the IH lesion via tray-delivered tooth whitening is critical prior to resin infiltration because once the resin has polymerised, it will be more impermeable and thus less likely to be modified by oxidative action. This case report describes an extended resin infiltration period under diminished ambient light prior to polymerisation that was required for aesthetic success.
CPD/Clinical Relevance: Ideal sequencing of treatment prior to resin infiltration is critical for physico-aesthetic success. The length of resin infiltration can be increased if results are not seen by the manufacturer-prescribed application time.
Article
The aesthetic appearance of the upper anterior sextant is a key determinant in the perceived attractiveness of a smile. It is characterised by a balance between both pink (gingival) and white (dental) elements.1 In a proportion of individuals, there is a defect in mineralisation of the organic matrix component during enamel development. Often, post-eruptive surface breakdown can lead to an increased incidence of hypersensitivity and susceptibility to caries formation. Incisor hypomineralisation is characterised clinically as white spot or combination white-brown lesions. These areas often are the source of anxiety during the expression of a smile, and can instigate negative social interactions especially among the younger population, thereby affecting confidence.
Incisor hypomineralisation is commonly classified as part of the molar–incisor hypomineralisation (MIH) spectrum, with the incidence in the northern European population ranging from 3.5% to 25%, with an average of 16%.2 Often, the mixed white and brown lesions are differentially diagnosed as fluorosis or Turner's hypoplasia.3 MIH differs from hypoplasia in that the former features a defect in mineralisation of the organic matrix, whereas the latter exhibits defective secretion of organic matrix during amelogenesis. The realm of hypomineralised lesions comprises both hypomaturation and hypocalcification. Histotypically, hypomaturation is rich in amelogenin, whereas hypocalcification is amelogenin-poor. MIH is categorised as a hypocalcified lesion, which additionally is albumin rich. Albumin is a protein normally excluded from the enamel matrix during formation because it impedes mineralisation; however, it is almost always present in hypomineralisation.4 There are proteins other than albumin that are naturally present during enamel matrix formation that regulate the size, shape and orientation of the crystals.5 In normal enamel development, enzymes work to progressively eliminate this protein content until the content is &1% by weight, and the space is occupied by tightly bound crystals.6 It is an ongoing conundrum as to how the secreted enamel matrix barrier is breached by albumin in MIH.
The period of susceptibility ranges from 32 weeks in utero to 5.5 years of age, that within which crown formation and calcification occurs.2 The aetiology of MIH has been postulated to be multifactorial, with factors such as maternal perinatal illness and medication use, premature birth, genetics, childhood fevers and ailments (e.g. asthma and pneumonia) being proposed.7
Biomechanically, there is a 50–75% reduction in both surface micro-hardness and modulus of elasticity relative to normal enamel. This is attributed to a 20% decrease in mineral content. The protein content of severe hypomineralisation lesions can be up to 15-fold that found in normal enamel.8 Conventional phosphoric acid etching produces a less distinct pattern on MIH-affected versus normal enamel, and results in a porous structure as the compromised foundation for the hybrid layer.9
Modalities for treatment
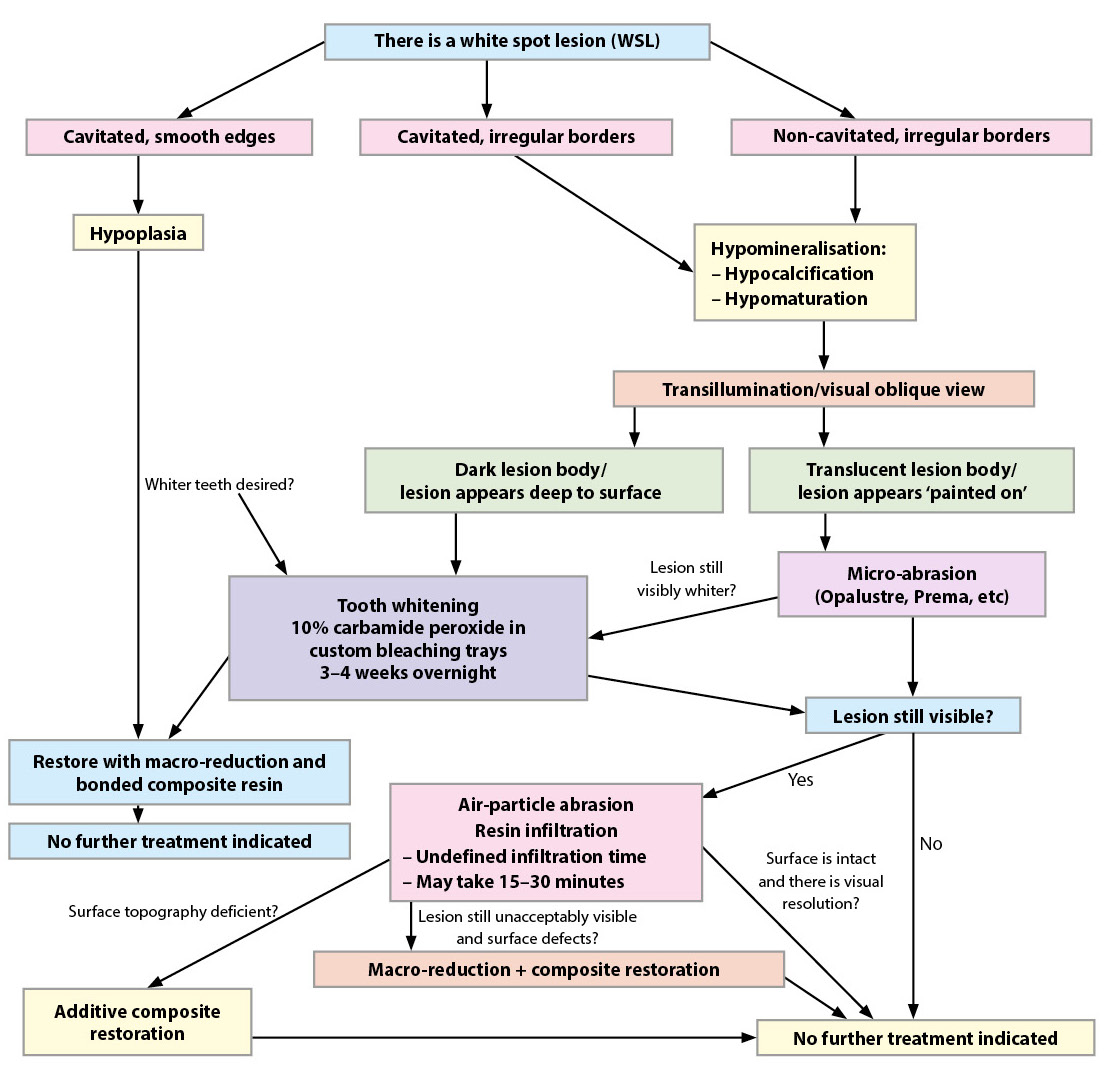
The visual disturbance and underlying structural deficiency in incisor hypomineralisation (IH) has led to the development of a protocol aimed at staging therapeutic interventions in a minimally invasive, graded approach for aesthetic and functional recovery (Figure 1).10
Figure 1. Protocol diagram.
Step 1: dental and/or lesion whitening
Dental whitening, featuring a 10% carbamide peroxide solution delivered in custom nightguard trays, has been well established in the literature.11 The breakdown of stain macromolecules as a result of free radical cleavage is as effective as that in sound, chromatic enamel and dentine, and is critical as a pre-prosthetic treatment in chromatic IH lesions.12 The ability to lessen or remove the yellow-brown dimension of these lesions is beneficial, and the simultaneous value-increase of the surrounding enamel often leads to improved camouflage of the IH lesion. Value is one of the three dimensions of colour used in dentistry. It refers to perceived brightness, with a higher value typically being brighter and lighter in appearance. Lopes et al reported no negative changes in enamel micro-hardness or morphology after a 10% carbamide peroxide solution was used over a 2-week period, whereas mild areas of erosive change were noted when a 3% hydrogen peroxide solution was used.13 Nonetheless, it is prudent to use a calcium-phosphate remineralisation paste (e.g. ToothMousse Plus, GC America) for a 2-week period post-whitening to maximise mechanical strength, because this represents the necessary refractory period to allow for oxygen radical dissipation prior to dental bonding procedures.
Dental whitening is always performed prior to the application of composite sealants to maximise its results: resin-sealed teeth are impermeable to oxidative radical penetration and efficacy.14 In the case of stained enamel opacities, the effectiveness of staging vital tooth bleaching prior to resin infiltration has been well established,15 and deemed critical because infiltration alone will not remove the chromatic aspect of the lesions, and will obviate future opportunities for whitening of the lesion.
Step 2: surface layer modifications
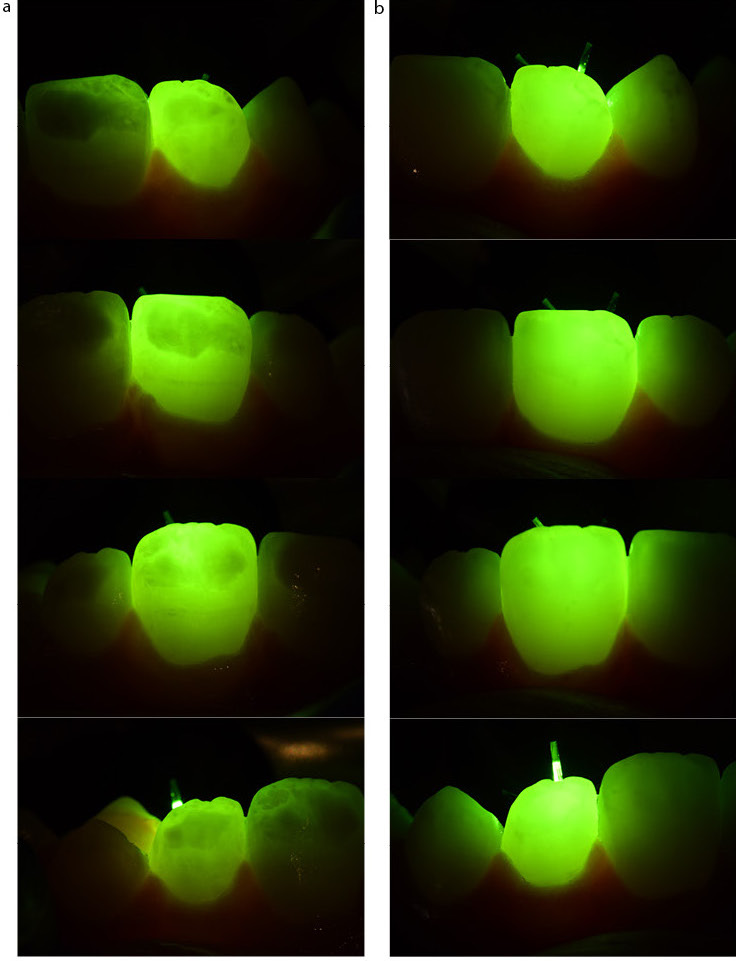
A consideration prior to infiltration is the physical depth of the lesion stratified in enamel, which can be characterised via transillumination and oblique visual observation.16 If the opacity appears translucent and light in nature when a light source is directed towards the facial surface from the palatal wall, the lesion will be located more superficially, distant from the dentino-enamel junction (DEJ). If the defect appears dark, the lesion is positioned closer to the DEJ, distant from the surface (Figure 2). This has the implication of a more unpredictable resin infiltration result. Transillumination has also been used by Marouane et al15 for intra-operative assessment of infiltration treatment progress and effectiveness. In the oblique visual observation technique, the lesion is viewed almost tangentially. As enamel is a glass-like substance, if the lesion appears to be painted on the surface, its position is superficial, and conversely deep, if visually sub-subsurface (personal communication, Prof David Manton, University of Melbourne).
Figure 2. (a) Transillumination showing pre-operative condition and mottled radiopacities. (b) Transillumination showing post-infiltration final result with significant resolutions of optical defects.
The irregular enamel prism arrangement of incisor hypomineralisation results in an irregular etch pattern and thus, erratic and variant depths of penetration by resin inflltration.17 Thus, if the lesion is deemed superficial, it is beneficial to remove the superficial enamel layer to gain both visual improvement and physical access to the deeper strata of the lesions. Micro-abrasion can be completed via both chemo-mechanical (e.g. Opalustre, Ultradent Products) and mechanical means (e.g. micro particle abrasion, Aquacare). If a longer refractory period between whitening plus micro-abrasion and resin infiltration is desired, the use of amorphous calcium phosphate–casein peptide creme (ToothMousse Plus, GC America) has been found to improve the appearance of white spot lesions over a 6-month period.18
Step 3: the concept of resin infiltration
The infiltration of white spot lesions is based on the premise that there are differing refractive indices between the intact enamel (RI: 1.62) and the lesion, causing a visual discontinuity. The lesion comprises regions that feature both water-dominant pockets (RI: 1.33) and air (RI: 1.00). The protocol calls for both the physical access into, and the desiccation of, the amorphous pockets within enamel, followed by a re-occupation of these spaces with a low-molecular weight resin monomer, triethylene glycol dimethacrylate (TEGDMA) (RI: 1.46). The replacement therapy by the monomer results in an instant chameleon effect and aesthetic improvement on the regions accessed. Although a certain degree of infiltration efficiency is also seen with larger resin monomers, such as bisphenol A glycidyl methacrylate (bis-GMA), TEGDMA has been shown to have the best potential of arresting white spot lesions of carious aetiology.19,20
Resin infiltration of IH is preceded by preparation of the amorphous enamel surface by both micro-abrasion and chemical erosion. The use of 15% hydrochloric acid applied for a 2-minute period has been demonstrated to almost completely remove the enamel surface layer and gain a deeper etch pattern into hypomineralised lesions when compared to 33% orthophosphoric acid.21 Although Subramanium et al22 demonstrated the depth of penetration by TEGDMA to be only 6.06 ± 3.03 µm on artificial normal-enamel surface-generated hypomineralised lesions, other surface studies have demonstrated penetration depths up to 54 µm.23 It must be noted that the variation of resin tag development is significant with MIH lesions, with the balance of favour tipping towards greater effectiveness in more superficial, accessible lesions. Crombie and Manton exhibited an average penetration depth of 670 ± 390 µm paired with an increase in micro-hardness of 1.0 ± 0.7 GPa, both beneficial for the optical and mechanical function of the affected teeth.24
Step 4: conservative reduction and layering
As some infiltrated IH lesions are recalcitrant to treatment, these cases call for conservative recontouring and composite stratification to mask the lesion and to restore surface impermeability. This is a last resort and is to be considered only when the above three modalities have been unsuccessful in visual correction of the lesion.
Case report
A 13-year-old ASA 1 healthy female presented to the practice with a chief concern of white spot lesions paired with yellow-coloured teeth (Figure 3). Clinically, the significant lesions were confirmed not to be of carious origin, with the appearance of yellow mottling within the lesion located on UR2. The visual contrast between the lesions and the surrounding dental tissue was high, with distribution of white spot lesions aesthetically limited from UR4–UL4 in the incisal half. Transillumination (Translume, ValoX, Ultradent Products) revealed lesions featuring a mottled mixed opacity, which indicated varying depths of stratification within the enamel body.
Figure 3. (a,b) Pre-operative views of the patient showing the incisor hypomineralisation.
Treatment options were discussed with the patient and mother, and a conservative protocol to treatment was confirmed, with a focus on minimally invasive progressive staging.
Tooth whitening was to be completed first, followed by a combination micro-particle abrasion treatment at the same time as the resin infiltration procedure, spaced 14 days apart to allow for oxygen radical dissipation. If the lesions were still visually significant to the patient at the end of these steps, then macro-reduction of the surface, dissection of the lesion and aesthetic composite layering was to be considered.
Digital intra-oral scans were taken (Primescan, DentsplySirona) after the final deciduous canine was removed, and printed models were used to generate positive-pressure-type custom bleaching trays. The informed consent included the knowledge that the bleaching trays were only fit for purpose during this single procedure because the patient's continuing dental development would quickly render the trays unusable in the future. The patient's baseline shade was Vita 2M1 (3D-Master, Vita Zahnfabrik) (Figure 4).
Figure 4. Baseline shade prior to tooth whitening: Vita 2M1 (3D Master, Vita Zahnfabrik).
The patient was prescribed the use of 10% carbamide peroxide (Opalescence, UT, USA) to be used overnight for 2–4 weeks until the maximal value correction was reached. Reassessment of the final achieved shade showed an improvement to the Vita 0M3 level for the cervical aspects of all teeth with reports of no-to-minimal intra-procedural sensitivity (Figure 5). A 14-day stand down period was observed, during which time ToothMousse Plus (GC America) was used nightly to optimise any aesthetic gains.
Figure 5. Post-whitening result: Vita 0M3 (3D Master, Vita Zahnfabrik).
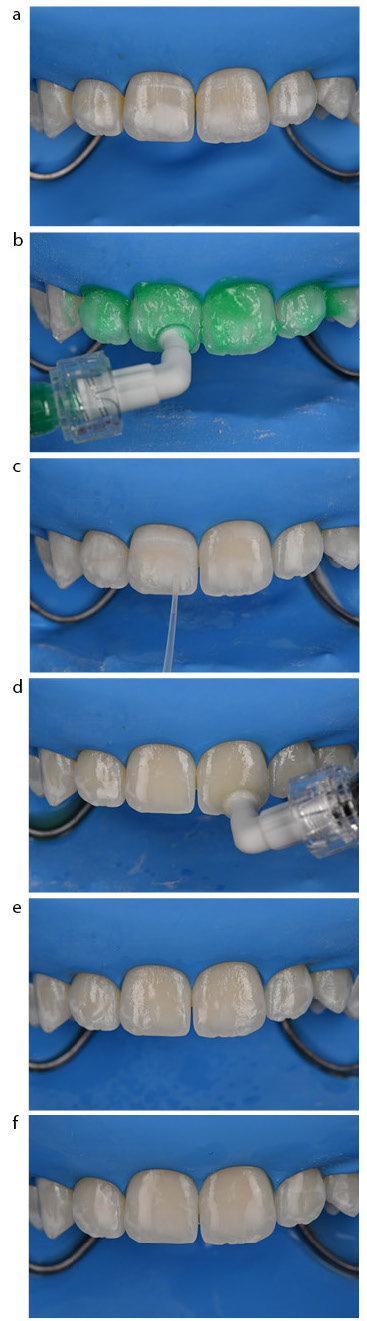
On the day of the resin infiltration procedure, absolute isolation with inverted rubber dam was used for the resin infiltration protocol to minimise any caustic effects on the soft tissue (Figure 6). Pre-treatment, micro-particle abrasion was carried out over all of the lesions (29-µm aluminium oxide, Aquacare UK) to remove any smear layer and to increase the surface area for treatment. Four cycles of the Icon-preparatory steps were executed as follows: 15% hydrochloric acid applied (Icon-Etch, DMG UK) for 2 minutes prior to rinsing and drying. Ethanol (Icon-Dry) was applied to the lesions for 30 seconds and air dried. Cycles 2 and 3 were preceded again by the use of micro-particle abrasion for 5 seconds per tooth as above in an attempt to remove superficial opacities and gain greater penetration to the white spot lesions. Cycle 4 did not feature pre-treatment by micro-particle abrasion. The resin infiltrant (Icon-Infiltrant, DMG UK) was used during the primary application for 17 minutes, alternating between passive and active (i.e. scrubbing and dabbing) modes.25 The lesion started to show significant chameleon resolution at the 12-minute mark, with changes plateauing around the 15-minute mark. The infiltrated surface was gently air dried and cured. A second soak of the resin infiltrate for 5 minutes to ensure uniformity of the surface was completed and cured.
Figure 6. (a) Initial isolation pre-procedure. (b) Application of Icon-Etch (15% HCl (aq)). (c) Application of Icon-Dry (ethanol). (d) Application of Icon-Infiltrant (TEGDMA). (e) Immediate post-infiltration result. (f) Post-finishing and polishing.
Any surface indentations that were present in the initial stage were subjected to bonding with a fifth-generation total etch bonding agent (Peak Universal, Ultradent) and 81% filled flowable composite application (Majesty Flow, Kuraray Noritake) prior to a full final cure with glycerine air barrier to eliminate the oxygen-inhibited layer. The surface was finished (Sof-lex, 3M) and polished (ASAP, Clinicians Choice) to high shine.
Immediate post-operative evaluation showed excellent resolution of the targeted lesions; however, peri-lesion regions of dehydration in the form of white streaks and spots were visible. The patient was reassured and dismissed. The reassessment appointment at the 1-week mark indicated successful resolution of virtually all significant white spot lesions with a visibly thrilled patient as the ultimate result (Figure 7).
Incisor hypomineralisation exhibits a wide range of surface layer depths and variable body depth.26 Superficial IH lesions may be subjected to enamel micro-abrasion with agents such as Opalustre (Ultradent Products) with minimal alteration in enamel roughness and wear.27 A variable success rate is observed with resin infiltration. Lesions that were pre-treated with air-particle abrasion alone and/or in combination with 5.25% sodium hypochlorite all showed similar, yet variable, penetration depths of infiltrant and thus, the latter agent was not employed in this case.28 The case presented exhibited significant opacity on transillumination, indicating a depth of lesion body distant from the surface – as such, surface chemo-micro-abrasion was not employed, as this step would only have a minimal effect on the result. Tray-delivered tooth whitening was completed using a 10% carbamide peroxide solution (Opalesence PF, Ultradent Products) for 3–4 weeks until maximal value was reached. The reason this approach was chosen over a high concentration hydrogen peroxide approach was because the latter exhibits significantly lower bonding strengths even after a 3-week refractory period post-whitening.29 Whitening at this pre-infiltration stage is important because the effectiveness of tooth whitening post-infiltration is impaired by the reduction in permeability, and thus if the patient were ever to have wanted the appearance of whiter teeth, the moment is now. Specific to the lesion, there is a side benefit of lightening chromatic aspects. A 14-day refractory period was observed following whitening to allow for maximal polymerisation effectiveness, which would otherwise been negatively affected by residual oxygen radical emission.30 Air-particle abrasion (APA) using a 29-µm aluminium oxide powder suspended in a 17.5% ethanol solution (Aquacare) was applied to the lesion surface prior to the preparation steps of the Icon (DMG America) resin infiltration system. The goal was to micro-roughen the surface layer and gain a more permeable surface for the 15% hydrochloric acid, which features first in the protocol. The acid acts to erode the surface layer to an average depth of 58 ± 12 μm per cycle.26 APA was used again prior to rounds 2 and 3 of the preparatory stage, again to facilitate greater depth of penetration into the lesion. In all rounds, ethanol (Icon-Dry) was applied for 30 seconds after removal of the 15% hydrochloric acid to wick moisture externally from the lesion.
The manufacturer of the system used (Icon, DMG) recommends a 3-minute initial infiltration step, light curing, followed by an additional minute of infiltrant application. The author purports that once the infiltrant has been cured, the surface will be then impermeable to further attempts at penetration. The case demonstrated above indicated that the visual resolution of the lesion did not start to occur until the 15-minute mark. Provided that the ambient or operating light in the dental surgery is low, there is no foreseen disadvantage for the increased ‘soak time’ of the infiltrant because this is the only opportunity for the resin to reach its maximum depth of penetration. The second infiltration step aims only to regularise or make the surface of the lesion uniform.
Studies have shown that conventional phosphoric acid etching also shows a milder etching pattern on hypomineralisation-affected enamel, hence the reason for increasing micromechanical retention via air-particle abrasion.31 If composite resin is to be added to the infiltrated surface, it is important that the surface be re-treated using an etch-and-rinse approach: this has yielded higher microtensile bond strengths relative to a self-etching adhesive.32
Indeed, when adding composite resin to an infiltrated surface, a greater proportion of favourable cohesive failures over unfavourable adhesive failures were noted for enamel surfaces that were treated with 15% hydrochloric acid, caries infiltrant and conventional total etch adhesive relative to 15% hydrochloric acid and caries infiltrant alone.33
The depth of penetration of the resin infiltrate is the final determinant of treatment success. Penetration may be limited by the presence of carbonate in MIH lesions, thus impeding access.34 Studies suggest that the application of 5% sodium hypochlorite may be able to increase shear bond strength to MIH lesions with certain adhesives;35 however, it is unknown whether the oxygen radicals formed via application will have a deleterious effect on the strength of the resin bond.36 Chay et al noted an increase in shear bond strength of hypomineralised enamel to resin composite with 5.25% sodium hypochlorite whether resin infiltrant was used or not.37
Wright9 proposed a technique using 5% sodium hypochlorite applied in multiple, 15–20-minute sessions as a pre-treatment to etch-and-rinse adhesives. It is a modality to deproteinise the lesion, expose a more ideal bonding substrate to resin infiltration and also functions to simultaneously whiten the IH lesion through oxidative action.9 Wright noted a period of aesthetic stability during his 5-year post-treatment observation period.
It is always prudent to observe a refractory period between such oxidising treatments and the infiltration procedure itself as a precaution to maximise bond strength.
Infiltration effectiveness is normally gauged by the application of ethanol in the preparatory steps leading up to actual infiltration. Visually, the borders of the lesion should appear muted in appearance and less distinct and be more reactive to the wet ethanol. If they do not readily respond, the author has incorporated the use of conservative micro-particle abrasion in an attempt to gain greater depth of access to these recalcitrant areas.
Future developments in resin infiltrant technology may include a pre-treatment 5.25% sodium hypochlorite step as well as the inclusion of remineralising and antibiotic agents that will act to biologically optimise the substrate concurrent with its occupation of enamel defects. An ideal system should allow for colour stability over time and feature surface shear bond strengths consistent with normal enamel and dentine. The protocol above reflects and amplifies the need to understand the pathophysiology of human dental defects fully in order to stage treatment protocols that can be applied in a minimally invasive manner; that which respects the mantra of responsible aesthetics.