Starcke EN The history of articulators: ‘scribing’ articulators: those with functionally generated custom guide controls, part I. J Prosthodont. 2004; 13:118-28 https://doi.org/10.1111/j.1532-849x.2004.04018.x
Starcke EN The history of articulators: ‘scribing’ articulators – those with functionally generated custom guide controls, part II. J Prosthodont. 2005; 14:57-70 https://doi.org/10.1111/j.1532-849x.2004.04045.x
Basudan TA, Alghaythi KS, Abuhabshah AA Iatrogenic damage in restorative tooth preparation and management. Int J Community Med Public Health. 2021; 8:3708-3712 https://doi.org/10.18203/2394-6040.ijcmph20212632
Shah YR, Shiraguppi VL, Deosarkar BA, Shelke UR Long-term survival and reasons for failure in direct anterior composite restorations: a systematic review. J Conserv Dent. 2021; 24:415-420 https://doi.org/10.4103/jcd.jcd_527_21
Wang X, Huyang G, Palagummi SV High performance dental resin composites with hydrolytically stable monomers. Dent Mater. 2018; 34:228-237 https://doi.org/10.1016/j.dental.2017.10.007
Eltahlah D, Lynch CD, Chadwick BL An update on the reasons for placement and replacement of direct restorations. J Dent. 2018; 72:1-7 https://doi.org/10.1016/j.jdent.2018.03.001
Caplin RL Dentistry – art or science? Has the clinical freedom of the dental professional been undermined by guidelines, authoritative guidance and expert opinion?. Br Dent J. 2021; 230:337-343 https://doi.org/10.1038/s41415-021-2726-4
Saunders WP, Saunders EM Prevalence of periradicular periodontitis associated with crowned teeth in an adult Scottish subpopulation. Br Dent J. 1998; 185:137-140 https://doi.org/10.1038/sj.bdj.4809750
Alharby A, Alzayer H, Almahlawi A Parafunctional behaviors and its effect on dental bridges. J Clin Med Res. 2018; 10:73-76 https://doi.org/10.14740/jocmr3304w
Pereira FJ, Lundh H, Westesson PL Morphologic changes in the temporomandibular joint in different age groups. An autopsy investigation. Oral Surg Oral Med Oral Pathol. 1994; 78:279-287 https://doi.org/10.1016/0030-4220(94)90055-8
Sutin AR, Terracciano A, Ferrucci L, Costa PT Teeth grinding: is emotional stability related to bruxism?. J Res Pers. 2010; 44:402-405 https://doi.org/10.1016/j.jrp.2010.03.006
Ohkawa S, Okane H, Nagasawa T, Tsuru H Changes in retention of various telescope crown assemblies over long-term use. J Prosthet Dent. 1990; 64:153-158
Hernigou P, Queinnec S, Flouzat Lachaniette CH One hundred and fifty years of history of the Morse taper: from Stephen A. Morse in 1864 to complications related to modularity in hip arthroplasty. Int Orthop. 2013; 37:2081-2088 https://doi.org/10.1007/s00264-013-1927-0
de Souza Costa CA, Hebling J, Randall RC Human pulp response to resin cements used to bond inlay restorations. Dent Mater. 2006; 22:954-962 https://doi.org/10.1016/j.dental.2005.10.007
Tan K, Ibbetson R The effect of cement volume on crown seating. Int J Prosthodont. 1996; 9:445-451
Nemane V, Akulwar RS, Meshram S The effect of various finish line configurations on the marginal seal and occlusal discrepancy of cast full crowns after cementation – an in-vitro study. J Clin Diagn Res. 2015; 9 https://doi.org/10.7860/jcdr/2015/12574.6283
de Freitas Oliveira J, Ishikiriama A, Vieira DF, Mondelli J Influence of pressure and vibration during cementation. J Prosthet Dent. 1979; 41:173-177 https://doi.org/10.7860/jcdr/2015/12574.6283
Carrotte PV, Johnson A, Winstanley RB The influence of the impression tray on the accuracy of impressions for crown and bridge work–an investigation and review. Br Dent J. 1998; 185:580-585 https://doi.org/10.1038/sj.bdj.4809870
Breitman JB, Nakamura S, Freedman AL, Yalisove IL Telescopic retainers: an old or new solution? A second chance to have normal dental function. J Prosthodont. 2012; 21:79-83 https://doi.org/10.1111/j.1532-849x.2011.00797.x
Niederman R, Badinovac R Is it philosophy of care or evidence-based dentistry?. Evidence-based Dent. 1998; 1:3-4
Anterior aesthetics without dysfunction: a case report. Part 2: the prosthodontic conversion Raj Raja Rayan Aesthetic Update 2025 2:1, 29-33.
Authors
Raj RajaRayan
OBE, MA (ClinEd), MSc, FDSRCS(Ed), FFGDP(UK), MRDRCS(Eng), MGDSRCS(Eng), DRDRCS(Ed), BDS, LDSRCS(Eng), Former Dean, FGDP(UK), RCS (Eng), Former Associate Dean, London Deanery; Recently, Professor and Head of Restorative Dentistry, College of Medicine and Dentistry; Former restorative referral-only practice in Harley Street; Honorary Colonel of The Commonwealth of Kentucky. Now retired
Marketing cosmetic dentistry is financially fashionable. Anterior aesthetic reconstructions are an art form showcasing the dental technician's skill. There is a perceived concern that anterior reconstructions that do not consider the functional features of the mutually protected occlusion may, in susceptible patients, lead to dysfunction with its possible consequences. Part 1 described a case in which severe anterior tooth wear was restored using compomers for the palatal surfaces, and composites anteriorly to provide acceptable aesthetics. The compomers were used so the patient could relatively easily fashion this ‘softer’ material during parafunction. This provided a pattern of anterior guidance within the patient's ability to adapt. Once adequate time was allowed to ensure the guidance was not dysfunctional, it was copied and replicated onto an incisal guidance table for future use. This article deals with the conversion of the guidance to fixed prosthodontic work.
CPD/Clinical Relevance: Transfer of anterior guidance; telescopic crowns and planning for failure.
Article
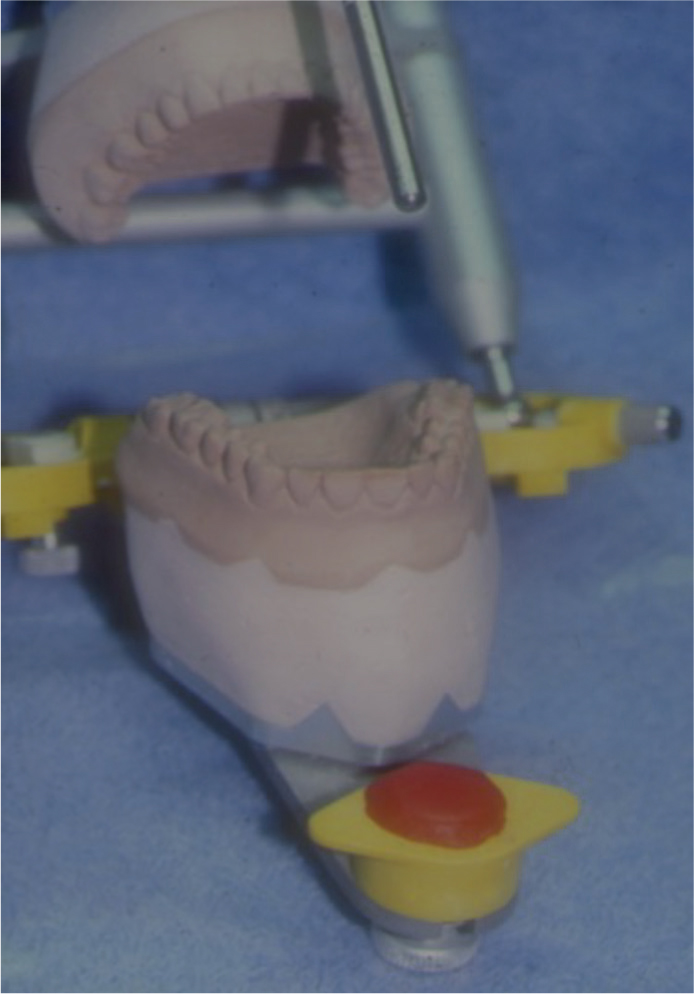
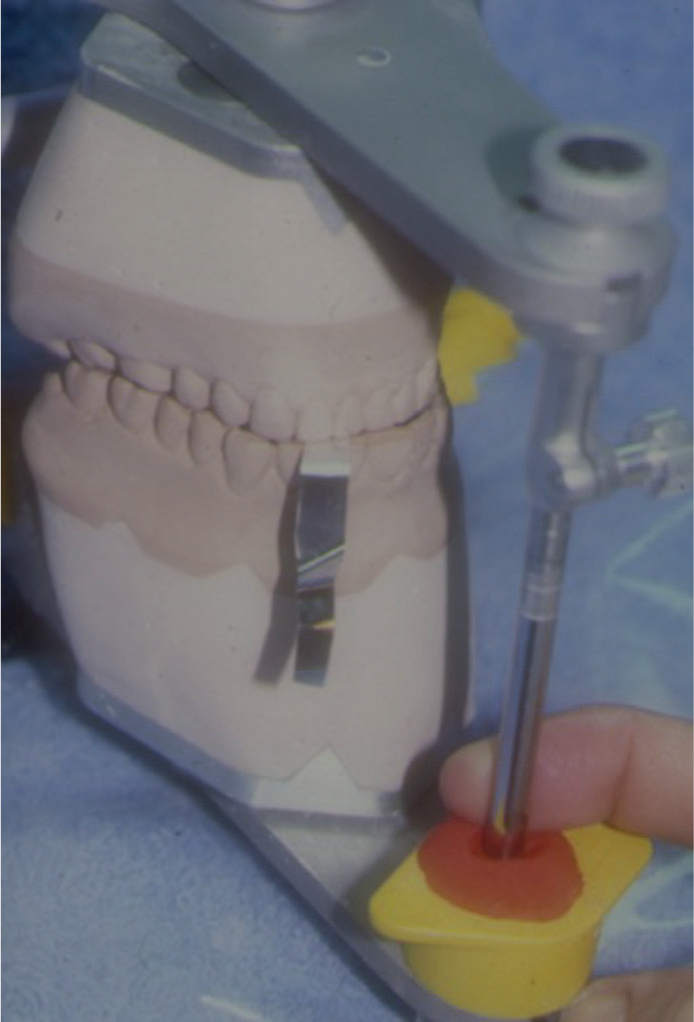
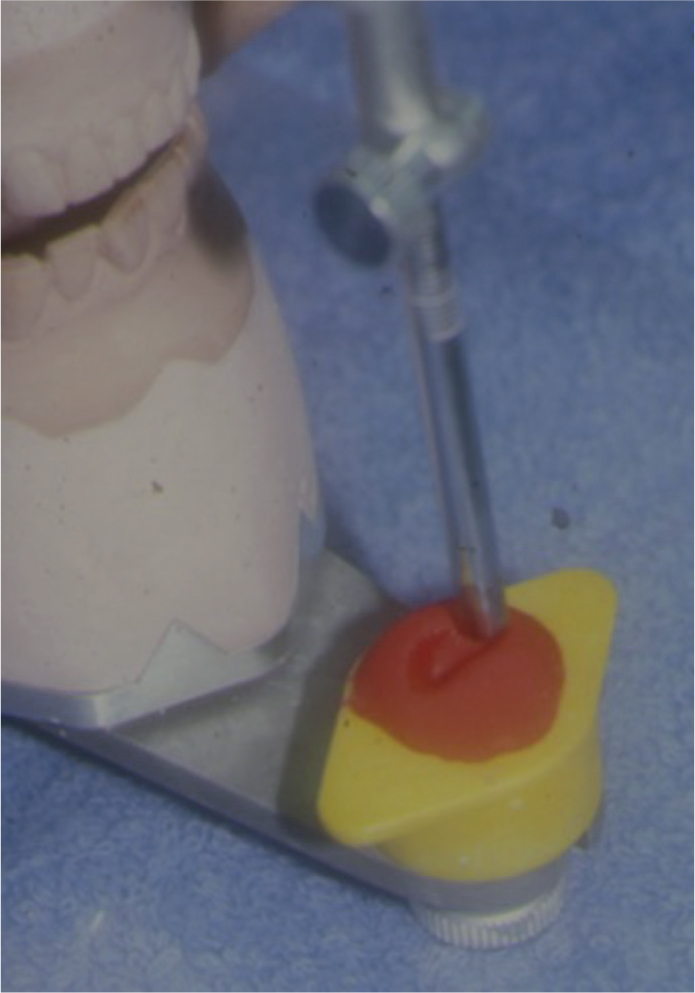
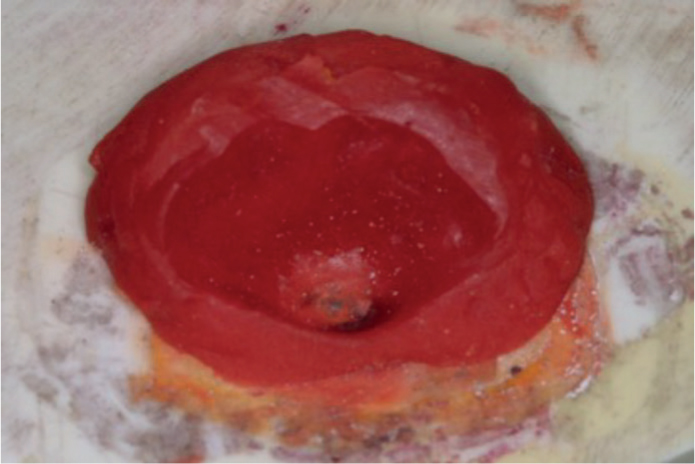
In the previous article, severe anterior tooth wear was restored using compomers (the material of choice of its time 30 years ago) for the palatal surfaces and composites anteriorly to provide acceptable aesthetics.1 The compomers were used so the patient could relatively easily fashion this ‘softer’ material during parafunction. This provided a pattern of anterior guidance within the patient's ability to adapt. Once adequate time was allowed to ensure the guidance was not dysfunctional, it was copied (Figures 1–3) and replicated onto an incisal guidance table (Figure 4) for future use. This article deals with the conversion of the guidance to fixed prosthodontic work.
Figure 1. Casts in intercuspal position.Figure 2. Incisal pin in unset acrylic.Figure 3. Teeth engrave guidance.Figure 4. Anterior guidance table.
The anterior guidance table
The provisional composite work had no signs or symptoms for over 3 months, and the occlusion was stable with posterior stability and anterior disclusion. Once stability was established, and the anterior guidance was within the patient's adaptive capacity, study casts were taken. These were mounted onto an articulator, and the anterior guidance of the provisional aesthetic restorations was transferred to an incisal guidance table.2 This was constructed by sliding articulated upper against lower casts, the envelope of motion of the incisal pin engraving the tooth guidance onto an acrylic mould block placed on the incisal table.3,4 The ensuing photographic illustrations (not the patient being discussed) are of a full mouth reconstruction where the impressions of the final provisional crowns are mounted on a SAM articulator (SAM Präzisionstechnik GmbH, Germany). Because the vertical dimension was changed and the SAM articulator has a straight incisal pin, the incisal pin must be mounted on the mandibular bow and the incisal table on the maxillary bow (upside down in contrast to manufacturer illustrations). If the pin is straight, when the vertical dimension is changed, the centric point of the pin in the acrylic will no longer be centred owing to the closing arc. Hence, it will not be centred in the guidance table. This is not a problem with the Denar articulator (Denar Mark II articulator, WhipMix, KY, USA), where the pin is curved to compensate for the change in height during the closing arc, thus keeping the centre point centred. Hence, in the Denar, the incisal pin remains on the maxillary bow when the vertical dimension changes.
The guidance copy technique is to place a newly mixed mass of quick-setting acrylic (Duralay pattern resin, Reliance Dental, Illinois, USA) onto the incisal table, with which it will bond. Then, the lubricated (Vaseline the tip) incisal pin is immediately dropped into it when in maximum intercuspation. Before the material sets, the anterior guidance of the palatal surfaces of the upper incisors is mechanically traced to indent the acrylic while it is still setting on the incisal table. Once set, the form of the guidance is indented permanently into the acrylic as the anterior guidance. This table with the acrylic indent can be used later with the final working casts.
The technician will also construct an upper vacuum- and pressure-formed splint blank with a 0.5-mm provisional cast thickness. When the upper anterior teeth are prepared, this cast can then be used to construct the temporary acrylic or bisacryl crowns.
Once the teeth were prepared, the working cast of the impression was mounted back in the same intercuspal position against the original lower cast. This was to reverse design the palatal contours of the upper crowns. The waxing of the palatals of the upper incisors was fashioned while the incisal pin remained in contact with the acrylic indent on the guidance table during motion. This way, the anterior guidance of the provisional composites was transferred to the definitive work.
The conundrum
The question today is whether to be conservative and maintain the long-term, repairable provisional restorations, or reconstruct the anterior teeth with new crowns with the associated substantial iatrogenic damage.5 While the case for the former is compelling, composite materials undergo many changes in the oral environment, including fractures,6 imbibitions of moisture, leaching of toxic material, staining of the filling, degrading of the resin7 including its change of colour and breakages in stages.8 Nevertheless, even when cured, composites are full of free radicals, so they can continue to be patched.
This case was undertaken 30 years ago when the concepts of minimally invasive dentistry,9 consequences of operator-induced damage and the ‘repeat restorative cycle’10 were not as well understood. The question then was, how soon would the patient like to have fixed prosthodontic work?11 Nevertheless, in hindsight, there are learning points from this case.
Crown lengthening
When fixed prosthodontics are chosen, in most cases of severe tooth wear, some crown lengthening surgery12 is required because any occlusal reduction could leave the pulp compromised as crown height for retention is obtained from this surgical tooth lengthening. In this instance, because of the Dahl technique, no pulp-compromising palatal tooth reduction was needed. This patient also had a thick biotype of periodontal support. Hence, no surgery was performed on this patient. Nevertheless, teeth prepared for crowns carry the risk of becoming non-vital.13
Planning for failure
Teeth that are already compromised with severe tooth wear are more likely to fail. Sound tooth destruction during preparation can be minimized and retention improved by using parallel-sided, rather than tapered, burs (Figure 5), such as the Brasseler Komet 878.314.012 FG diamond and finished with the matching H283.314.012 FG TC bur (Komet, Germany), as in this case. Because teeth with tooth wear are relatively short, for additional retention and resistance to rotation, resistance slots (Figure 7) using a Jet FG Tungsten Carbide (Kerr Dental UK) 170L bur (Figure 6) were placed. This too will compound the risk of pulpal damage and should be undertaken with caution, while conforming to the parallelity of the single-draw crown preparations (Figure 8).
Figure 5. Chamfer bursFigure 6. Jet 170L for slotsFigure 7. Labial view of the tooth preparations.Figure 8. Occlusal view of the tooth preparations
Hence, the first potential failure will be the future endodontic needs of these substantially prosthodontically over-prepared teeth. Therefore, retrievability and re-use of expensive dentistry should be pre-planned.
The second failure would be the displacement of a crown or crowns during parafunction14 as anterior guidance continues to remodel. This can be due to many reasons. These include adaptation when posterior teeth fail or are restored, and the occlusion changes. This patient had several missing posterior teeth, and some of those remaining were heavily restored. When posterior stability is compromised, anterior guidance attempts to compensate. Another possibility is that the temporomandibular joint (TMJ), the disc assembly and the glenoid fossa undergo changes with age and pathology, and ther is a shift in the mandibular movement.15 The muscles of mastication alter the way in which they function to compensate for such changes. Patients are also reported to clench and parafunction as part of changes to their lifestyle challenges.16
The third potential failure is that the patient travels from afar and would find it difficult to return frequently.
Linking crowns and multi-abutting will mean that each crown will support the other. However, this has been suggested as false security. It is because each tooth has a range of physiological mobility, owing to the resilience of the periodontal ligament during function and parafunction. As these mobilities differ from tooth to tooth, this differential, while retaining one crown under stress, could unseat another. The unseating of a crown that is linked to other crowns will be difficult to detect. Back siphonage of infective biological and other materials into the now micro unseated crown will cause pathology to the exposed tooth preparation. It is for this reason that double or multi-abutting teeth are frowned upon.
In summary, the potential for problems of future endodontics, the need for definite work to continue to remodel with physiological or pathological changes to the occlusion and a formula for recovery and retrievability of the work should be built in.
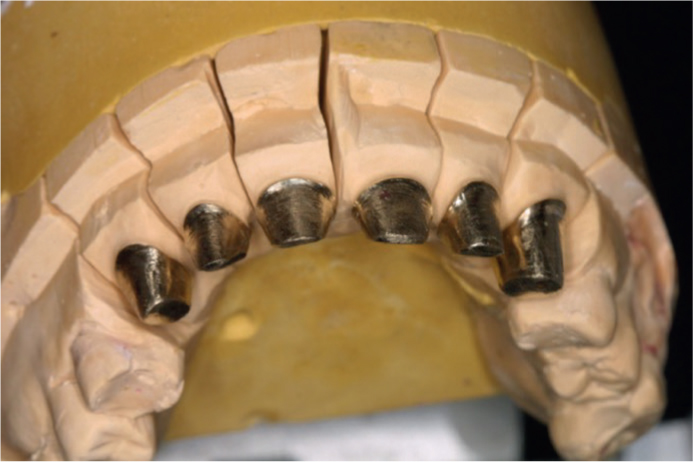
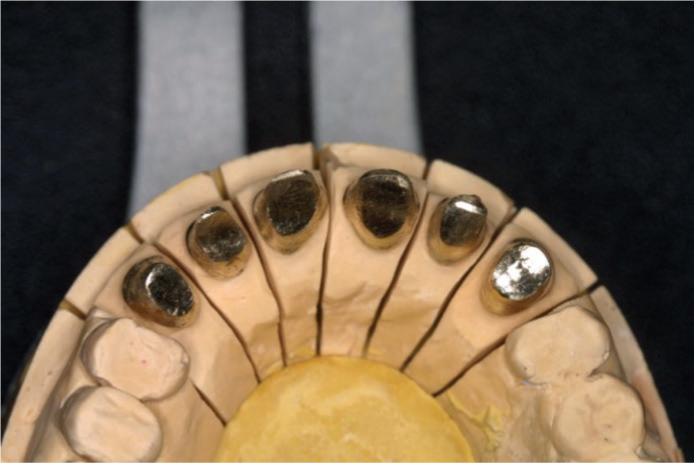
The solution was to construct gold copings17 on the teeth made parallel to one another and have telescopic crowns18 placed over them (Figure 9). These would have a 6° taper,19 which is an optimal angle for an overcasting to fit against, similar to the concept of a Morse taper20 (Figure 10). The marginal finish would be a chamfer because this would allow burnishing of the metal margins. It is important to note that this ‘double crown’ technique is hugely destructive of tooth substance as one needs space for the copings and more space for the aesthetic crowns.
Figure 9. Gold copings for telescopic crownsFigure 10. Copings parallel to each othe
These copings would be cemented with a definitive cement. The cement would be a superfine particle zinc phosphate cement (Fleck's zinc phosphate cement, Mizzy, USA), the material of choice 30 years ago. This is technique sensitive and, if incorrectly applied, would be traumatic to the pulp owing to its high acidity. Nevertheless, it has the smallest particle size of any definitive cement and reportedly produces the best fit. Glass ionomer is another option. Resin cements are to be avoided as the resin is hazardous to pulp owing to its petrochemical products.21 As they also contain filler particles, they form the thickest cement lute,22 making them unsuitable for such precise cementation where the relationship of one coping to another is critical. Anything that can alter it will affect the relationships of the final castings.
Cement is applied sparsely at the margin only. Any greater load of cement will travel up the preparation and clog the occlusal surface to prevent the coping from seating fully.23 This is more important when the preparations are more parallel.24 A vibrating technique when seating will produce the best results.25 If endodontic treatment were to be needed in the future, the coping would be perforated to enter the root canal. Following root treatment, the coping could be resealed with a long-lasting operative material.
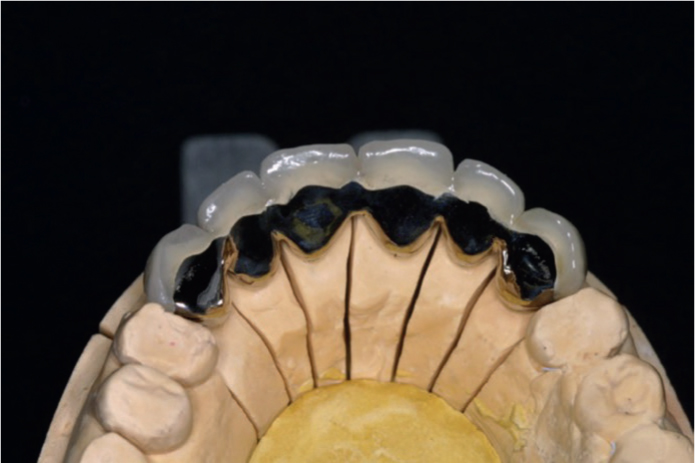
The crowns were of a high gold content alloy bonded to porcelain, where porcelain was only in the aesthetically visible labial areas. The relatively softer gold was palatal and copied the established anterior guidance. As gold is a malleable and ductile material, it would continue to remodel and burnish as and when time and function-related occlusal changes occur. These crowns would be linked. There are additional problems with the type of tray used,26 the thixotropic nature of the impression material and the differential mobility of teeth when linking crowns. They include the intrusive forces of the impression where one prepared tooth is intruded less than another, further compounded by the errors when separating the dies and the reseating of the dies,27 where the relative accuracy of one preparation to another is more compromised. There are various ways to mitigate this when there is a need to link crowns, such as:
Try in the copings, link them with a metal rod and quick-setting acrylic. Pick this up in a new impression. Replace the dies into the copings. Construct a solid model and use this as the basis for the linked crowns. Figure 11 demonstrates this from a full-mouth reconstruction case after healed crown lengthening and for making provisionals.
Construct the metalwork of the crowns, without the porcelain, as individual units. Place the individual metal copings in the mouth, link them with a rigid metal rod and quick-setting acrylic and then pick up a new impression. Construct a solid model, solder the metal crowns together and then apply the porcelain. This technique is used when the metal has a lower gold content, and soldering or welding temperatures would damage the porcelain if it had been completed.
In the present case, copings were constructed, tried in, and had the single unit aesthetically porcelained and completed crowns on the same dies. The completed single crowns were placed individually over preparations. These crowns were picked up as a single unit using the same technique of a rigid rod and quick-setting acrylic. These crowns were then transferred to a solid cast of a refractory model (Figure 12), and the crowns were post-ceramically soldered. This latter technique allows for the assessment of the aesthetics and function. It also enables the clinician to make minor modifications to almost the final work to be accomplished and then pick it up as a single unit. As the author used a high gold content alloy, the solder was a low-temperature fusing material that would not damage the porcelain. The solder could be polished to become one (the photograph is not of this case, but a post ceramic pick up was used to solder the last molar to the bridge).
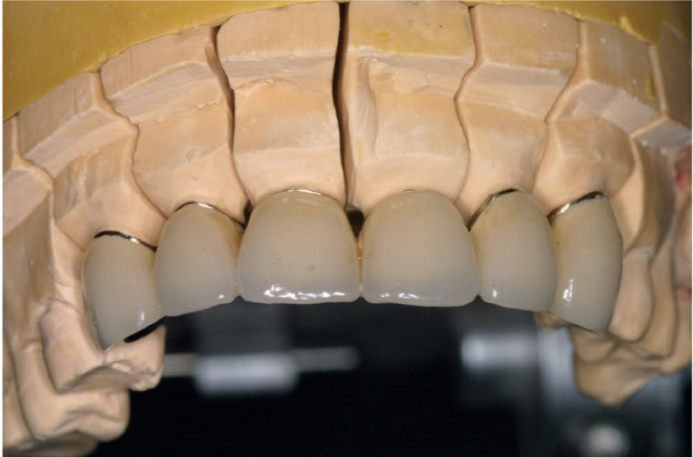
These linked crowns (Figures 13 and 14) would be cemented with a provisional cement for retrievability and recementation,28 usually zinc oxide with nogenol with modifier (TempBond NE; Kerr Corp, Orange, Ca, USA). In the future, should any debond, the tooth underneath was already protected by the cemented coping. When needed, this could be easily removed for access to the copings, or when laboratory adjustments were required (Figure 15).
Figure 13. Anterior view of the linked crowns.Figure 14. Palatal view of the crowns. Note the gold palatals.Figure 15. The anterior six crowns.
As with all the author's patients, this patient was referred for specific work. The patient, both during and after treatment, was returned to the referring practitioner for routine, uncomplicated, continuing care. When the work was concluded, the author recalled them at increasingly longer intervals to review the prognosis.
Reflection
Today, it would have been unlikely to have hastened the fixed prosthodontic treatment when so many beautifully aesthetic, better adhesive and more durable composites are available. Not least of all, there has been the relentless retraining of dentists to reduce the potential for iatrogenic damage that my well-meaning generation undertook. Enter today, the era of minimally invasive dentistry and trust in the holistic ability of patients to recover without destructive mechanical interventions.
Nevertheless, there are so many re-treatments needed from yesteryear's invasive dentistry that some aspects of this treatment approach and thought processes might be useful to draw from – be it positive or negative. This case appears to have stood the test of time.
With regard to the field of occlusion, far too many philosophies once thought to have been common-sense practice, have proven to be anything but sensible. The lack of compelling evidence-based research29,30,31 is an indictment on the academic profession, as this has been a field evoking great passion and argument for more than 100 years. It is time to get our scientific evidence together without the need to sacrifice so many patients on the altar of ‘what I believe’.