Segundo ÂRTC, Saraiva S, de Castro C CAD-CAM natural restorations: reproducing nature using a digital workflow. J Esthet Restor Dent. 2023; 35:993-1000 https://doi.org/10.1111/jerd.13028.
Nohl FS, Steele JG, Wassell RW Crowns and other extra-coronal restorations: aesthetic control. Br Dent J. 2002; 192:443-450 https://doi.org/10.1038/sj.bdj.4801396
Coachman C, Calamita MA, Sesma N Dynamic documentation of the smile and the 2D/3D digital smile design process. Int J Periodontics Restorative Dent. 2017; 37:183-193 https://doi.org/10.11607/prd.2911
Bakti I, Santosa AS, Irawan B, Damiyanti M Chameleon effect of nano-filled composite resin restorations in artificial acrylic teeth of various shades. J Phys Conf Ser. 2018; 1073 https://doi.org/10.1088/1742-6596/1073/5/052011
Rosentritt M, Hartung J, Preis V, Krifka S Influence of placement instruments on handling of dental composite materials. Dent Mater. 2019; 35:e47-e52 https://doi.org/10.1016/j.dental.2018.11.010
Marquardt W, Seiss M, Hickel R, Reichl FX Volatile methacrylates in dental practices. J Adhes Dent. 2009; 11:101-107
Sananez A, Sanchez A, Davis L Allergic reaction from dental bonding material through nitrile gloves: clinical case study and glove permeability testing. J Esthet Restor Dent. 2020; 32:371-379 https://doi.org/10.1111/jerd.12546
Misra S, Daly B, Dunne S Dentist– patient communication: what do patients and dentists remember following a consultation? Implications for patient compliance. Patient Prefer Adherence. 2013; 7:543-549 https://doi.org/10.2147/PPA.S43255
Van Meerbeek B, De Munck J, Yoshida Y Buonocore memorial lecture. Adhesion to enamel and dentin: current status and future challenges. Oper Dent. 2003; 28:215-235
Abbasi M, Moradi Z, Mirzaei M Polymerization shrinkage of five bulk-fill composite resins in comparison with a conventional composite resin. J Dent (Tehran). 2018; 15:365-374
Biradar B, Biradar S, Ms A Evaluation of the effect of water on three different light cured composite restorative materials stored in water: an in vitro study. Int J Dent. 2012; 2012 https://doi.org/10.1155/2012/640942
McCollum BB Function-factors that make mouth and teeth a vital organ. J Am Dent Assoc. 1927; 14
Schuyler CH Principles employed in full denture prosthesis which may be applied to other fields of dentistry. J Am Dent Assoc. 1929; 16:2045-2054
Biradar B, Biradar S, Ms A Evaluation of the effect of water on three different light cured composite restorative materials stored in water: an in vitro study. Int J Dent. 2012; 2012 https://doi.org/10.1155/2012/640942
Stuart CE The contributions of gnathology to prosthodontics. J Prosthet Dent. 1973; 30:607-608
D'Amico A Canine teeth-normal functional relation of the natural teeth of man. J South California Dent Assoc. 1958; 26:6-23
Schuyler CH The function and importance of incisal guidance in oral rehabilitation. 1963. J Prosthet Dent. 2001; 86:219-232 https://doi.org/10.1067/mpr.2001.118493
Stuart CE, Stallard H Principles involved in restoring occlusion of the natural teeth. J Prosthet Dent. 1960; 10:304-313
Nyman S, Lindhe J Considerations on the design of occlusion in prosthetic rehabilitation of patients with advanced periodontal disease. J Clin Periodontol. 1977; 4:1-15 https://doi.org/10.1111/j.1600-051x.1977.tb01878.x
Shillingburg HT, Sather DA, 4th edn. Chicago, IL, USA: Quintessence; 2012
Seligman DA, Pullinger AG The role of functional occlusal relationships in temporomandibular disorders: a review. J Craniomandib Disord. 1991; 5:265-279
Mehta S, Banerji S The application of occlusion in clinical practice part 1: Essential concepts in clinical occlusion. Dent Update. 2018; 45:1003-1015
Dzingutė A, Pileičikienė G, Baltrušaitytė A, Skirbutis G Evaluation of the relationship between the occlusion parameters and symptoms of the temporomandibular joint disorder. Acta Med Litu. 2017; 24:167-175 https://doi.org/10.6001/actamedica.v24i3.3551
Shillinburg HT, Wilson EL, Morrison JTChicago, IL, USA: Quintessence; 2000
Rieder CE Use of provisional restorations to develop and achieve esthetic expectations. Int J Periodontics Restorative Dent. 1989; 9:122-139
Gough MB, Setchell DJ A retrospective study of 50 treatments using an appliance to produce localised occlusal space by relative axial tooth movement. Br Dent J. 1999; 187:134-139 https://doi.org/10.1038/sj.bdj.4800223
Hemmings KW, Darbar UR, Vaughan S Tooth wear treated with direct composite restorations at an increased vertical dimension: results at 30 months. J Prosthet Dent. 2000; 83:287-293 https://doi.org/10.1016/s0022-3913(00)70130-2
Anterior aesthetics without dysfunction: a case report. Part 1: the operative dental procedure Raj Raja Rayan OBE Aesthetic Update 2025 1:3, 137-142.
Authors
Raj Raja RayanOBE
MA (ClinEd), MSc, FDSRCS(Ed), FFGDP(UK), MRDRCS(Eng), MGDSRCS(Eng), DRDRCS(Ed), BDS, LDSRCS(Eng), Former Dean, FGDP(UK), RCS (Eng), Former Associate Dean, London Deanery; Recently, Professor and Head of Restorative Dentistry, College of Medicine and Dentistry; Former restorative referral-only practice in Harley Street; Honorary Colonel of The Commonwealth of Kentucky. Now retired.
Marketing cosmetic dentistry is financially fashionable. Anterior aesthetic reconstructions are an artform showcasing the dental technician's skill. There is a perceived concern that anterior reconstructions that do not consider the functional features of the mutually protected occlusion, may, in susceptible patients, lead to dysfunction with its possible consequences. This series of three articles examines the restoration of worn upper anterior teeth with a plan for failure.
CPD/Clinical Relevance:
The mutually protected occlusion.
Article
Occlusion is a confusing subject. That is because, historically, occlusal philosophies were invented by well-intentioned, strong personalities and passionate operators promoting complicated and exacting prosthodontic procedures without any evidence based on science. The evolution of its understanding has been by philosophical experimentation, using sophisticated tools and unfortunate patients. Engineering concepts often superseded the physiological ability of such patients, often leading to pathological consequences. Occlusion has developed cult following with fixed ideologies of operating procedures and the potential for overtreatment of patients. Many eminent individuals in the field suffer from cognitive dissonance. If occlusion was the one important feature behind temporomandibular disorders, dentist would have, by now, cured this problem.
Today, the profession has moved away from the dogma of full mouth reconstructions, constructed to centric relation and balanced articulation, to one of the mutually protected occlusion. While the science for this later concept of anterior guidance and posterior stability is sparce, it is nevertheless, the current perceived wisdom. It is based on a biomechanical model that purports to reduce traumatic forces associated with the susceptible clenching parafunctionist.
Raison d'être
The purpose of this article is to suggest a simplified approach to demonstrate developing the anterior guidance on a patient with severe anterior tooth wear, prior to aesthetically reconstructing the smile. It includes a plan against future failure and litigation.
Patient visit
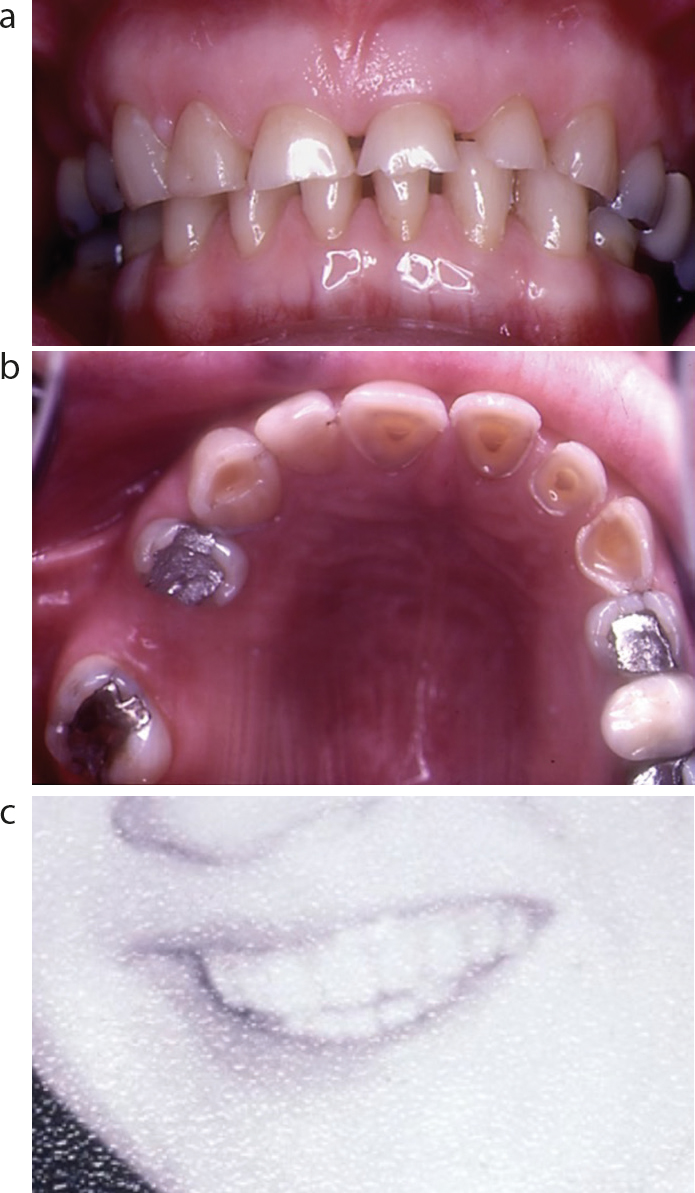
A 51-year-old female patient was referred for severe tooth wear of her upper front teeth (Figure 1). The aetiology was from being a youth of the flower power generation, leading to excesses in life, including alcohol consumption and its frequent ejection. The patient had long since put her past behind and was now immersed in conventional life with family. She was not concerned with her teeth, but her children had persuaded her otherwise. Patients are encouraged to bring a younger photograph of their smile (Figure 1c) when their teeth were relatively pristine. The teeth were vital, and radiographs showed no pathology. There was no periodontal disease and the bone quality was good. Her health did not exclude any dental treatment.
Figure 1.
(a,b) Frontal and occlusal views at presentation. (c) The patient's smile in her teens.
Occlusally, there was posterior stability with a definite habitual occlusion (maximum intercuspal position (ICP)), although the anterior guidance had been eroded away. Temporomandibular joint (TMJ) examination was in keeping with her age, with no symptoms or signs of derangement.
As the patient had travelled a long way and had no concept of what aesthetics may be achieved, an instant ‘mock-up’ of what a possible aesthetic result ‘could be’ was undertaken. While today it is expedient to digitize 3D smile designs and print out the models,1 this case was undertaken 30 years ago, and the tools available were diagnostic wax-ups with the technician,2 or a chairside mock-up by the clinician. It is not sensible to make 2D photographic enhancement into a 3D perspective.3 The mismatch between illusion and reality will lay the clinician open to litigation based on misrepresentation of the expectation of the final 3D result from a 2D photograph.
Chairside 3D mock-up
The chairside mock-up uses the abundant wasteful stock of expired composites in whichever type or shade that gets accumulated in a practice. It cannot be used on patients, but can be on models. Given that the composites' most endearing feature is its metamerism (chameleon effect),4 all shades will eventually equalize under a shadow.
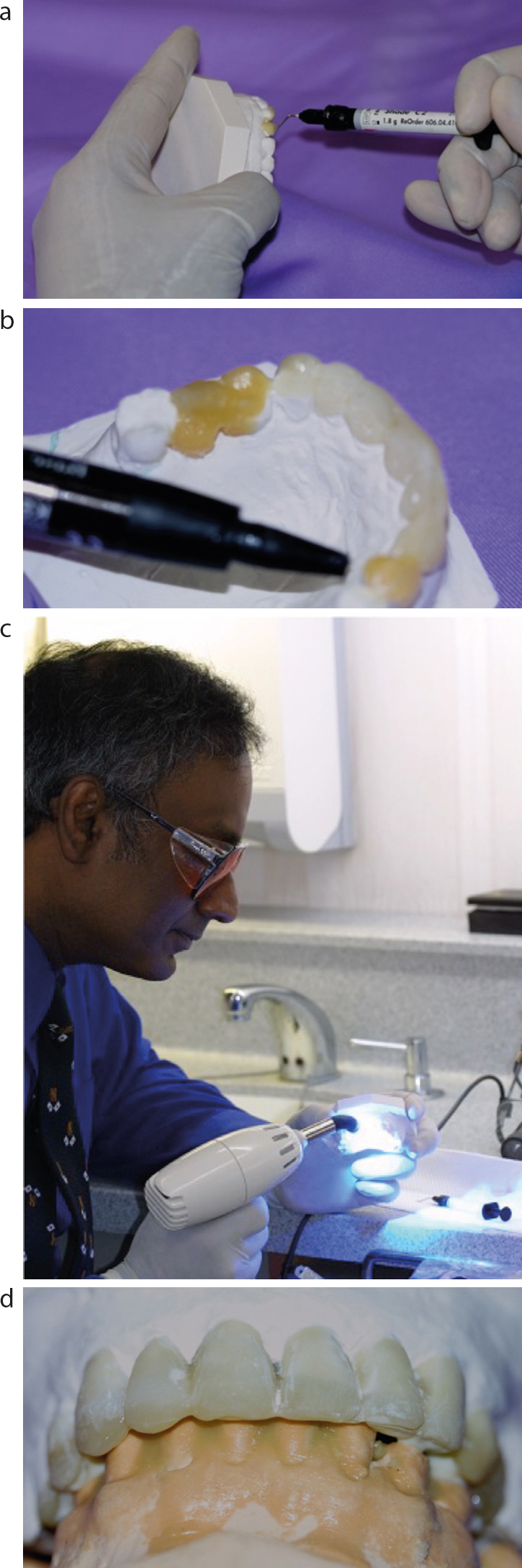
A quick setting plaster study cast of the patient is the foundation on which to build up the composite mock-up. Use flowable, tubed or compules of composites with a coated (e.g. Teflon) flat plastic to model the teeth freehand on the plaster cast. Noncoated modelling instruments of stainless steel will stick to composites. The composite filler particles will sandpaper the steel and incorporate metal particles into the finished product, ruining the aesthetics.5
Do not touch the unset composite even with gloved hands, as composites are potential allergens6 whose free radicals are able to penetrate gloves.7 Before curing, hand occlude and machinate together with the lower cast to establish posterior tooth contact. Ensure the upper anterior palatal build-ups ‘fit’ into the lower teeth (Figure 2). Build this in increments with 3-second light cure between placements (Figure 2c). To shape the cured crowns, use scalpel blades numbers 11 and 12 (Swann-Morton, Sheffield, UK) (Figure 3). Do not use rotating burs as they flatten the aesthetics. This is a truism even when modelling composite restorations on patients. Finish with flexible sandpaper discs, reversing the abrading side and always drawing towards you. This will help maintain the shape.
Figure 2.
(a) Using expired any type composite or compomer. (b) Use any colour material. (c) Just 3-second cures. Protect eyes. (d) Machinate lower cast for best bite before cure.Figure 3. Number (a) 11 and (b) 12 blades.
This process is quick and needs an artistic eye. Once completed, use an appropriate separating medium (Silicone release spray) and construct a vacuum and pressure-formed splint blank of 0.5 mm thickness of the composite mock-up (Easy-Vac, Prestige Dental UK). Perforate incisal edges with a sharp probe so that air is excluded when bulk filled.
Presenting to the patient
As the composite mock-up was created with different dispensed types and shades of the material (Figure 4a), when presenting it to the patient, to evoke its chameleon quality, place a hand over the gingival part for a shadow effect over the diagnostic work (Figure 4b). This will invoke its metameric properties and the shades will blend into a pleasant aesthetic.
Figure 4.
(a) Finished chairside mock-up. (b) Shadow of hand blends metameric composites.
Although this might impress, patients cannot truly judge what dentistry might look like in the end. Their politeness should be taken as informed, but not understood, consent.8 Hence provisional restorations are used to verify form, function and aesthetics.9 If the provisional work is liked and functions without failure, then copying it into the final restorations is both a recipe for success and a barrier to litigation.
In this case, temporary restorations were used before constructing provisional restorations. By definition, temporary restorations are just temporary and have, in contrast to provisional restorations, a simple transient message to convey.
Temporary restorations
Patients usually appreciate diagnostic mock-ups. For better appreciation they should be allowed to try it at home. A dramatic way of doing this is to fill the pressure formed, splint blank template with new composite of matching shade. Fit it over the patient's unprepared teeth getting them to bite and chew into it (Figure 5). Once a semblance of reasonable aesthetics and occlusion is created, light cure the bulk composite. Take a palatal putty impression.
Figure 5. Teate filled with bulk composite (unexpired!)
Composites are not naturally chemically adhesive. The way they bond to enamel is by micro-mechanical shrinkage,10 a physical bond caused by the change in dimension of the setting composite locking onto the etched rete pegs of the enamel. In this instance, there is no prepreparation of the teeth. As the composite is in bulk, there is greater macro-mechanical shrinkage11 causing the composite, as it changes dimension, to lock onto the teeth (Figure 6). Scalpel blades are used to remove the excess and to modestly shape the composite bulked teeth. The patient is informed that this is temporary, the occlusion is incorrect, it is a ‘take home and try out trial’. As it will fall out in bits, a return appointment is made the same week.
Figure 6. Now trim aesthetics with scalpel blades.
It has been my experience that good aesthetic reconstructive dentistry merges into the patient's persona and generally goes unnoticed. Hence, even this modest attempt is unlikely to elicit a response from family and friends as love overlooks beauty. A family member's less-than-ideal physical attributes, such size, shape and defects are generally ignored in a loving environment. So, the temporary aesthetic ‘fix’ is unnoticed at the beginning. However, composites readily imbibe moisture,12 and with usage, the material will start to fail. This is when the patient realizes that the original teeth, now visible between the breakages, have been severely aesthetically compromised. The cathartic marketing associated with the anterior reconstruction is now within the grasp of the patient.
The aesthetics now forms understood consent. What remains is to ensure that the functioning of the impending crowns do not cause a dysfunction of the occlusion during parafunction.
Anterior guidance or anterior interference?
The historic fashion for full mouth dentate prosthodontic reconstructions to be constructed to balanced occlusion13,14,15 was practised for several decades at the beginning of the last century, and perhaps even before the last millennium.16 Balanced occlusion is the simultaneous and equal contacts maintained among opposing tooth surfaces throughout the entire arch and throughout the entire excursion during function. This procedure was littered with failure on dentate patients and was eventually questioned.17,18 A newer fashion of canine guidance,19 incisal guidance,20 and the mutually protected occlusion21,22 came into the restorative culture without the necessity for using the centric relation position.23 This is current practice on dentate patients.
The exceptions are for edentulous complete denture cases24 and, more recently, reconstructions on periodontally compromised patients with the shortened arch.25 These cases default back to balanced occlusion. This is for practical convenience to prevent dislodging of full–full dentures during bruxing, or increasing the mobility of periodontally compromised and physiologically mobile teeth in the shortened arch.
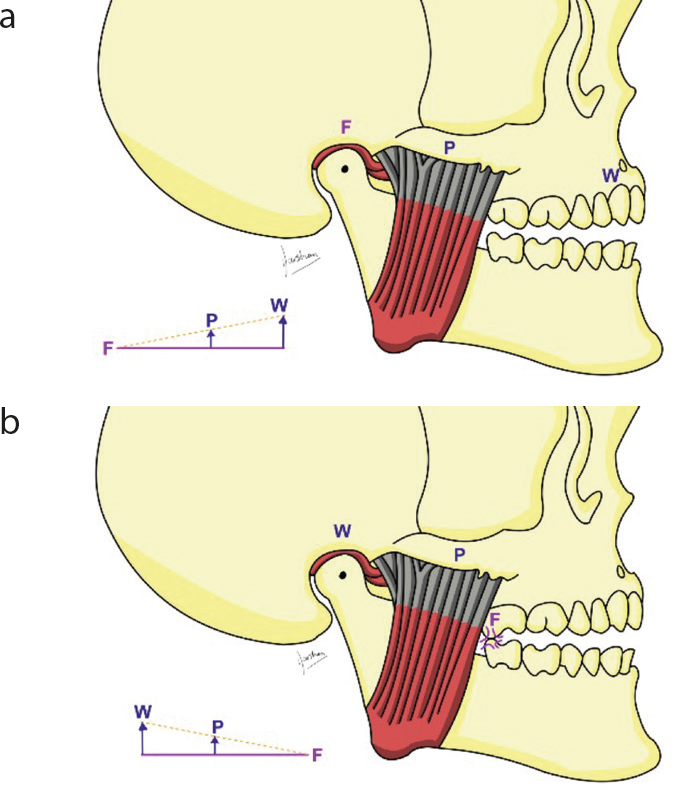
In anterior guidance, canines have the longest roots. The biomechanical rationale speculates that the mandible follows the principles of a Class III lever with the load being reduced by distance from the fulcrum (TMJ) and ‘proprioceptive thresholds and concomitant reflexes reduce the load’.26 As all patients parafunction, and past research fails to show any lasting effects in healthy individuals,27 healthy parafunction becomes the goal. What this means is that if the region of the temporomandibular joint (TMJ) is the fulcrum, the muscles of mastication, the generators of the parafunctioning forces, then the loads created on the most anterior teeth to disclude in parafunction will be far less (Figure 7a) than any load created nearer the muscles of mastication. Hence parafunctioning with anterior disclusion produces the smallest forces on teeth to dissoclude in this model.28
Figure 7.
(a) Mandible as class III lever. Fulcrum is TMJ. (b) Interference of tooth is fulcrum point.
A further complication is that if a posterior tooth is prematurely contacted, the Class III lever could transfer the fulcrum to the point of contact, and unexpected forces would be translated to the TMJ (Figure 7b).29 Whatever the science of this, it remains unproven in evidence-based medicine. In the absence of any other model that has not failed, this perceived clinical wisdom is followed to mitigate during litigation when a patient who had once adapted, becomes susceptible to TMJ dysfunction following dentistry. As this is currently taught universally, it is prudent to simulate this model when possible.
Nevertheless, this concept of canine guidance, the cornerstone of anterior guidance, was challenged recently (2021) in the article ‘Canine guidance on crowned teeth: time for a rethink?’.30 The authors analysed a 10 million-restoration dataset from National Health Service (NHS) Dentistry, concluding that in the case of the crowned canine, referred to as the ‘cornerstone of the arch’, it was the worst performing restoration at 15 years to time of extraction. They questioned traditional recommendations that canines should be placed into canine guidance and concluded that ‘If clinicians wish to prolong the life expectancy of an upper canine tooth, they must try to avoid crowning it’. While concluding correctly that patients were better off when their natural-shaped canines were allowed to function, they may have overlooked the lack of laboratory prescription by dentists in the NHS. In the NHS, and perhaps in the hands of many other practising dentists, the canine is prepped and replaced with an ad hoc dysfunctional guidance invented by the technician without an occlusal prescription. Therefore, these canines are not in guidance, but in newly created interference. As most are in porcelain or hard alloy, they are unforgiving in parafunction. Hence, they may have been prone to failure as the ‘corner tooth’ is now dysfunctional, rather than the original canine that was in physiologically functioning guidance. Evidence-based research is needed to conclude this debate, in the absence of which, establishing anterior guidance prevails for medico-legal reasons is prudent.
Establishing new anterior guidance with provisionals
When the patient returns with the partly fractured temporary work, it is an almost given that they would be keen to progress with the aesthetic improvement. While the technician can provide a beautiful smile, the prescription for the functional form of the lost palatal guidance will need to be re-established.
There are many ways to achieve this, many of which the author has routinely used, including taking kinematic facebow records and adjusting the anterior guidance to escape condylar movements,31 or using an adjustable anterior guidance table,32 or using prefabricated various value incisal tables,33 among many others.
Nevertheless, all these approaches always lead to the construction of long-term provisionals in ‘soft’ palatal material, such as acrylic or bis-acrylic. The patient continues to parafunction and ‘wear’ this into a comfortable and self-adapted palatal form that functions within the patient's adaptive capacity. This is then copied into the final occlusal scheme, usually, via a customised anterior guidance table.34
In this instance the following approach was used. The patient, while having severe past tooth wear on anterior teeth (Figure 1), had no signs or symptoms of TMJ dysfunction or discomfort. This indicated a patient who had easily adapted and one who was likely to adapt to the new occlusal scheme. If there was a problem, this is a reversible procedure.
The principles were:
To aesthetically create the smile with a reversible solution.35
To add a ‘Dahl’ appliance36 on the anterior teeth to create space for future castings. Composite materials are now considered a good alternative37 to the original laboratory-made cobalt–chromium cemented on the palatal of teeth.
The patient to ‘wear-in’ the provisionals long term and parafunction, while shaping the palatal surfaces to their adaptive capacity.
To eventually replicate the acquired adaptive guidance into future definitive work, and to allow final castings to continue to adapt to natural physiological changes including the regular remodelling of the TMJ assembly.
To plan for failure.
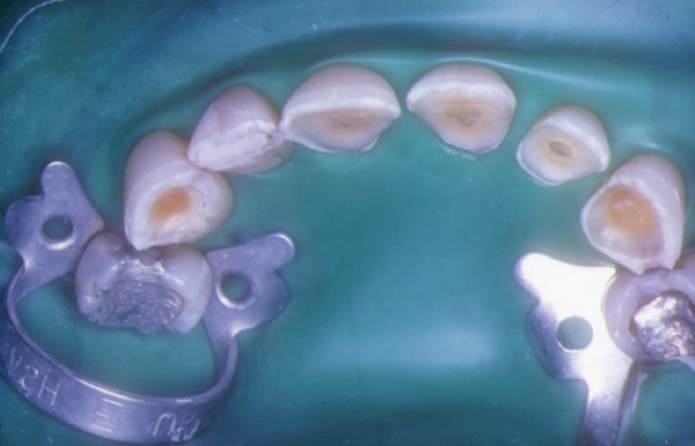
Rubber dam was applied to the anterior teeth (Figure 8). The previously kept palatal putty index was trimmed to fit over the dam and onto the teeth to form a template (Figure 9). Following a traditional acid etching procedure, the space between the putty template and the surface loss of palatal surfaces of the upper six anterior teeth were filled with a compomer. A compomer (polyacid modified composite resin) was used as this is ‘softer’ than a composite and the material of choice 30 years ago. It has fewer abrasive filler particles and long-chain tertiary amine resins for greater flexibility and adaptability. These materials have lower Young's modulus, allow for longer plastic deformation, making them less brittle than a composite and a tougher material from its adaptability. Nevertheless, compomers also have a sandpaper effect owing to, although much reduced, fillers. Hence, for patients who may be clenching parafunctionists where tooth surface loss was due to abrasion rather than erosion, it should be used with caution as the material will sandpaper down the opposing natural teeth – although to a lesser degree than a composite.
Figure 8. Rubber dam prior to procedure.Figure 9. Putty index used for palatal profile.
Once the palatal form has been fashioned (Figure 10), it provides the backplate from which to design the anterior aesthetics. For this, a colourmatched composite resin is used. As the base material of both compomers and composites are similar, these materials a will naturally bond to each other. The composites are built with cones, using an adapted ’PKT’ technique38 where the developing tooth's mamelons would have been (Figure 11). The space between these cones will be underfilled with a lighter shade of composite. Finishing is with scalpel, sanding discs and silicone rubbers and diamond polishing paste. The contrast of differing shades along with the undulation of the materials between the standout cones and the underfilled infill areas allow the light to reflect and refract in ways that make the restorations aesthetically pleasing. This also allows operator and patients to achieve aesthetic expectations.39
Figure 10. Palatal compomer build-up with index.Figure 11. Anterior composite build-up with cones.
Once minor occlusal adjustments are made for relative comfort, the work is left ‘high’ and the patient sent home. It is usual to observe this work for at least 3 months. (Figure 12).
Figure 12.
(a) The patient at presentation and (b) following the transitional composite makeover.
If there are no symptoms or signs of pathology, the restorations do not fracture or fail and the occlusion re-established by intrusion of the overfilled ‘Dahl’ teeth and eruption of the posterior teeth with associated alveolar compensation, then the work is probably stable for the next stage. Studies show the Dahl concept's objectives are reached in over 94% cases and the space is created irrespective of age and gender.40,41
Now one waits for at least 3 months without signs or symptoms to give time for parafunction to fashion the palatals, while the occlusion re-establishes.
Conclusion
Composites have greatly improved over the thirty years since the original case was undertaken. At the time of this treatment though, this technique was considered interim and diagnostic and a step towards prosthodontic intervention. Today, this case would have ended at this point and the patient reviewed regularly until such time as more aggressive treatment was indicated.
In the next part, the operative dental work will be converted to fixed prosthodontic treatment. The ethics, pros and cons as well as a modus operandi that was followed for this patient will be presented.