Liaw JJ, Park JH, Wang SH Interdisciplinary management of orthodontic-dental implant-restorative patients. Br Dent J. 2024; 237:379-388 https://doi.org/10.1038/s41415-024-7779-8
Yu X, Teng F, Zhao A Effects of post-extraction alveolar ridge preservation versus immediate implant placement: a systematic review and meta-analysis. J Evid Based Dent Pract. 2022; 22 https://doi.org/10.1016/j.jebdp.2022.101734
Jung RE, Ioannidis A, Hämmerle CHF, Thoma DS Alveolar ridge preservation in the esthetic zone. Periodontol 2000. 2018; 77:165-175 https://doi.org/10.1111/prd.12209
Zhuang J, Wang Y, Song Y The application of individualized abutment-crown integrated provisional restoration in optimizing the peri-implant soft tissue contour in the esthetic zone. J Esthet Restor Dent. 2021; 33:560-566 https://doi.org/10.1111/jerd.12726
Al-Harbi SA, Edgin WA Preservation of soft tissue contours with immediate screw-retained provisional implant crown. J Prosthet Dent. 2007; 98:329-332 https://doi.org/10.1016/S0022-3913(07)60107-3
A multidisciplinary approach for superior aesthetic outcomes in complex dental treatments Andrew Legg Andrew Flett Colin Campbell Aesthetic Update 2025 2:1, 35-39.
Authors
AndrewLegg
BDS MFDS RCS Ed, Dental Surgeon; The Campbell Clinic, Nottingham, UK
A multidisciplinary approach in the management of a complex dental case is described for a patient who required the replacement of a failing, malpositioned maxillary central incisor. The collaboration of orthodontists, oral surgeons and restorative specialists was important in addressing this case where functional, aesthetic and structural challenges converged.
CPD/Clinical Relevance: This article demonstrates how communication between specialties can give the best possible outcome for a patient.
Article
The management of complex dental cases often necessitates a multidisciplinary approach to achieve the best possible clinical outcomes. A multidisciplinary team (MDT) combines the expertise of various specialities, allowing for comprehensive diagnosis, treatment planning and execution tailored to the patient's unique needs.1 The collaboration of orthodontists, oral surgeons and restorative specialists is particularly critical in addressing cases where functional, aesthetic and structural challenges converge.2
This article presents a case of a patient who required the replacement of a failing, malpositioned maxillary central incisor. The tooth, traumatized during childhood, presented significant aesthetic and functional challenges, including poor alignment, compromised root development and an unfavourable prognosis. Through a co-ordinated treatment plan involving orthodontic alignment, ridge preservation and implant reconstruction, the MDT approach facilitated the creation of a stable and aesthetically pleasing result.
Case presentation
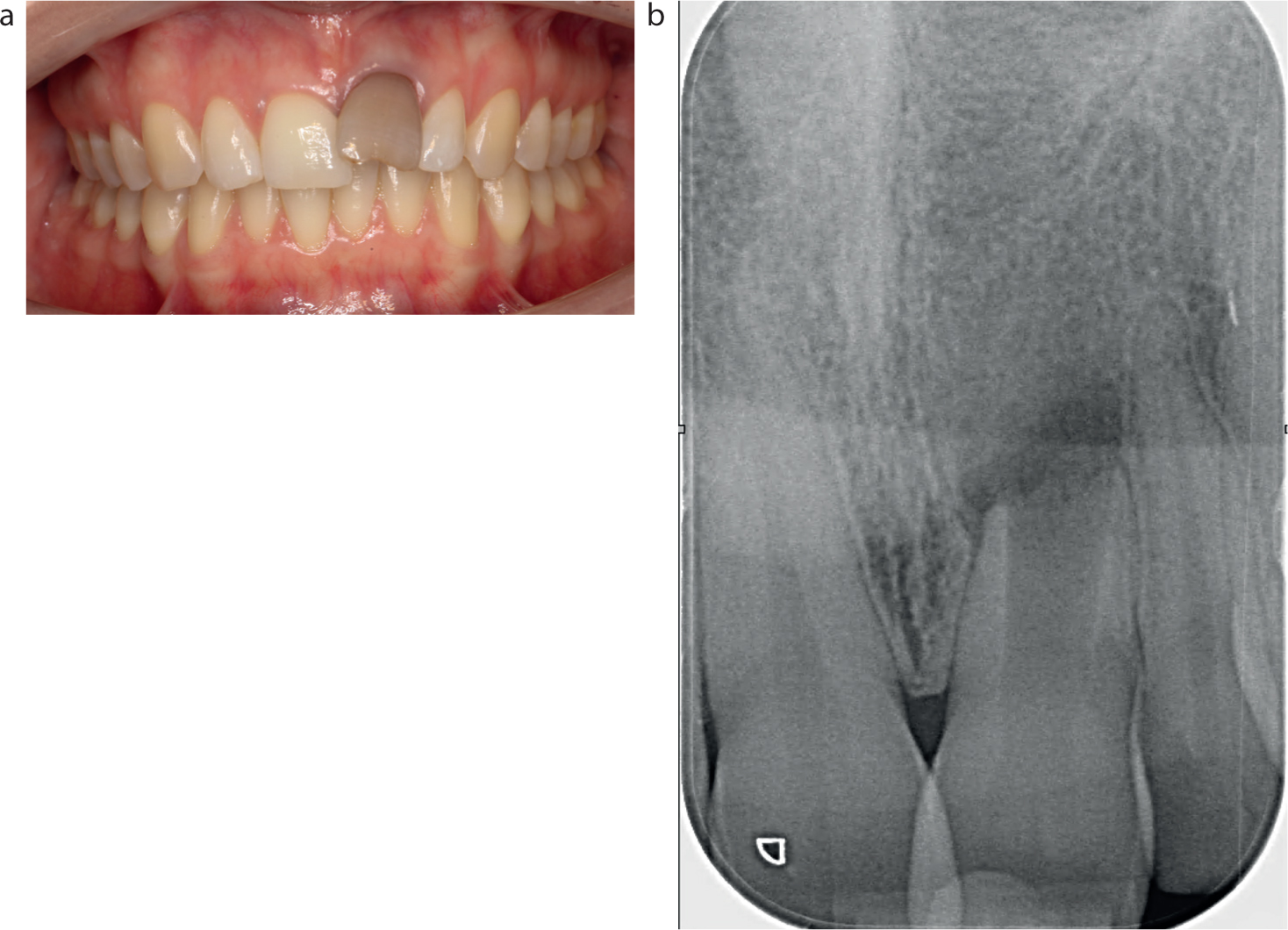
A 28-year-old patient who was unhappy with their dental appearance presented to the the practice. The patient had fallen over as a child, 20 years previously, and had traumatized the erupting UL1. As a consequence, this tooth never fully erupted, was high in the alveolus and was grey in colour (Figure 1). Owing to the delayed presentation, the UL1 had become crowded out of the arch form. Radiographs showed the UL1 to have an open apex with arrested development of the tooth root. The root length was around 50% of its comparator, the UR1 (Figure 1).
Figure 1. The patient presented with a traumatized UL1 that was (a) high in the alveolus and discoloured, and (b) had a reduced root length compared to UR1.
While percussion testing was not conclusive as to whether the UL1 was ankylosed, it was felt at initial presentation that the tooth was likely to be ankylosed owing to its position, appearance and history of traumatic intrusion. The prognosis of the UL1 was terminal, such that even if it could be aligned, it would not be a viable unit in the long term for root canal treatment and bleaching owing to its radiographic presentation.
From an orthodontic perspective, the patient presented with a Class II division 1 incisal relationship on a Class II skeletal base. They had an increased overjet of 8 mm from the UL1 (5 mm from the UR1), with moderate crowding of 5 mm in the upper arch and 3 mm in the lower arch. The buccal segments were a ½ unit Class II on the canines and molars bilaterally. It was also noted that both the UR2 and UL2 were diminutive at initial presentation. The patient requested orthodontic treatment to reduce the increased overjet and allow for prosthetic replacement of the failing UL1.
Treatment plan
The proposed treatment was spilt into sections as follows:
Open 9–10 mm space for an implant in the UL1 position (equal to UR1 size);
Create 1 mm of space mesially and distally around UR2 and UL2 for composite build-up of these teeth;
Treat to Class I canines and incisors and Class II molars.
To achieve these objectives, the decision was made to extract the UR4 and UL4 to re-create the necessary space and retract the upper labial segment teeth, reduce the overjet, and create space for the build-ups.
Owing to the complexity of the case, it was decided to treat the case using upper ceramic (3M clarity, .22x.28 MBT prescription, 3M, USA) and lower metal (AO mini master series .22x.28, MBT prescription, AO mini master series .22x.28 MBT prescription labial fixed applicances, American Orthodontics, USA) labial fixed appliances.
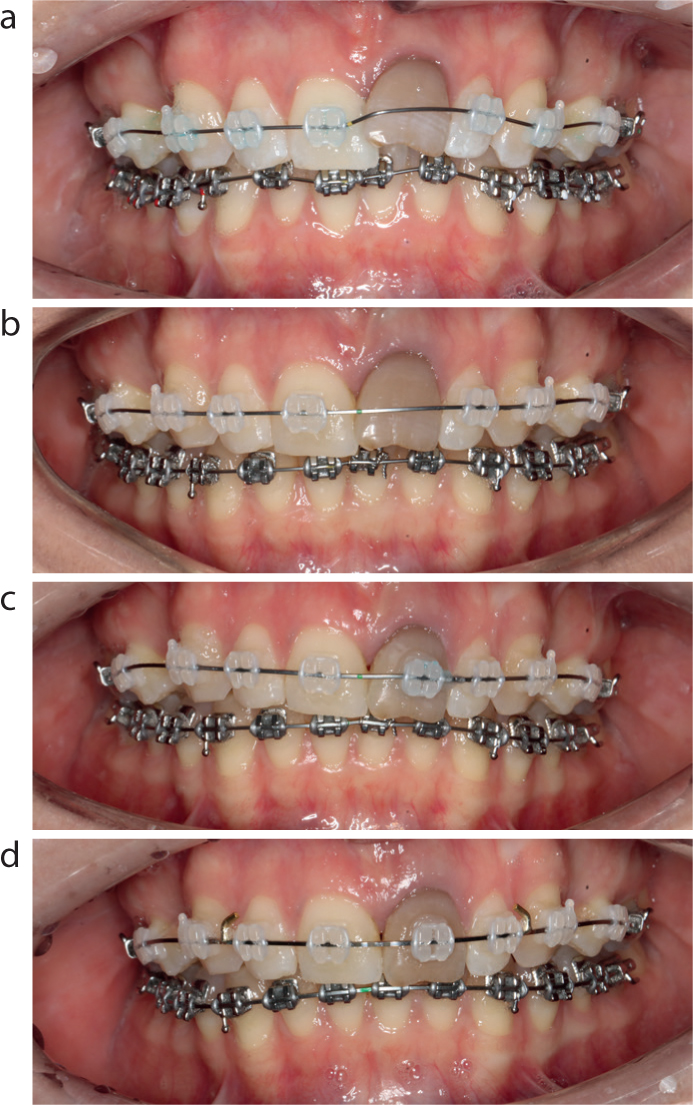
Active orthodontic treatment commenced after extraction of the UR4 and UL4. Over fears that the UL1 was ankylosed, and the risks of intrusion of the upper labial segment teeth that could occur if this was the case, UL1 was not bonded up (Figure 2). However, after the first visit, it was apparent that the tooth was not ankylosed because it had passively moved down as a result of the labial force of the nickel titanium archwire on its labial surface. This was fortuitous, because the implant team had been concerned about the gingival margin at initial presentation. From an implant perspective, achieving symmetry of the ginigval contour is essential for an aesthetic outcome. If the tooth had been ankylosed, then significant hard/soft tissue augmentation would have been required.
Figure 2.
(a) UL1 was not initially bonded up, (b) but moved down with the force of the archwire. (c,d) Hence, UL1 was then bonded up for alignment.
After one adjustment, the UL1 was picked up on the upper appliance and then used as its own space maintainer. Again, initially it had been felt that this tooth would have to be extracted mid treatment and a plastic prosthesis put onto the archwire to maintain the required space and aesthetics. However, this was not required during treatment (Figure 2).
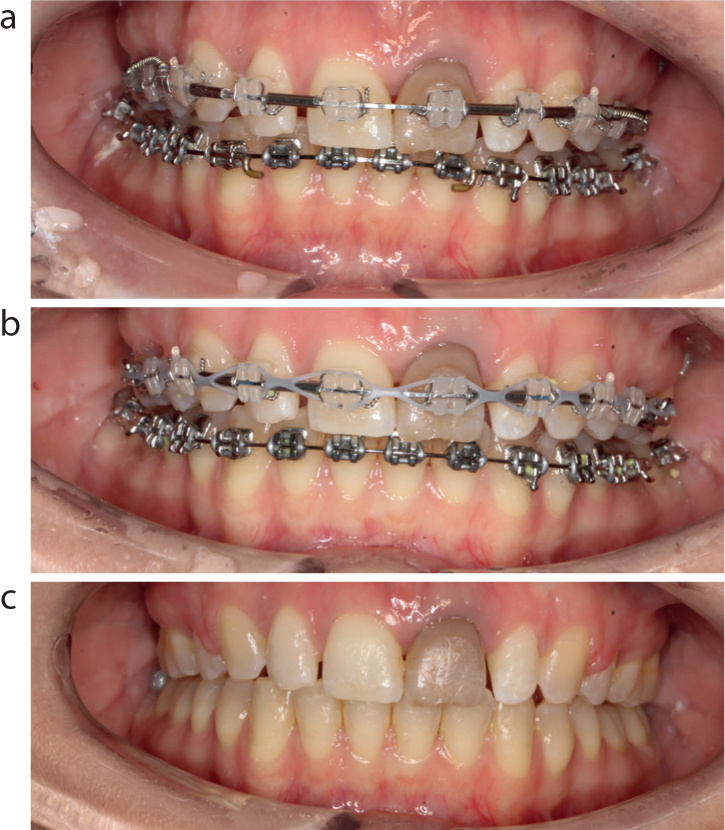
Orthodontic treatment then progressed until full alignment of the arches was achieved. Space at both sides of the upper lateral incisors was then opened up for the planned restorative treatment (Figure 3). At completion of active orthodontic treatment, the results were retained using upper and lower Essix C+ retainers. Owing to upper arch spacing, a bonded retainer was also placed between the upper central incisors.
Figure 3.
(a) Reduction of overjet and opening up space for composite build-up of UL2 and UR2, (b) followed by power chain for final upper centre line correction (c) and at debond.
Ridge preservation
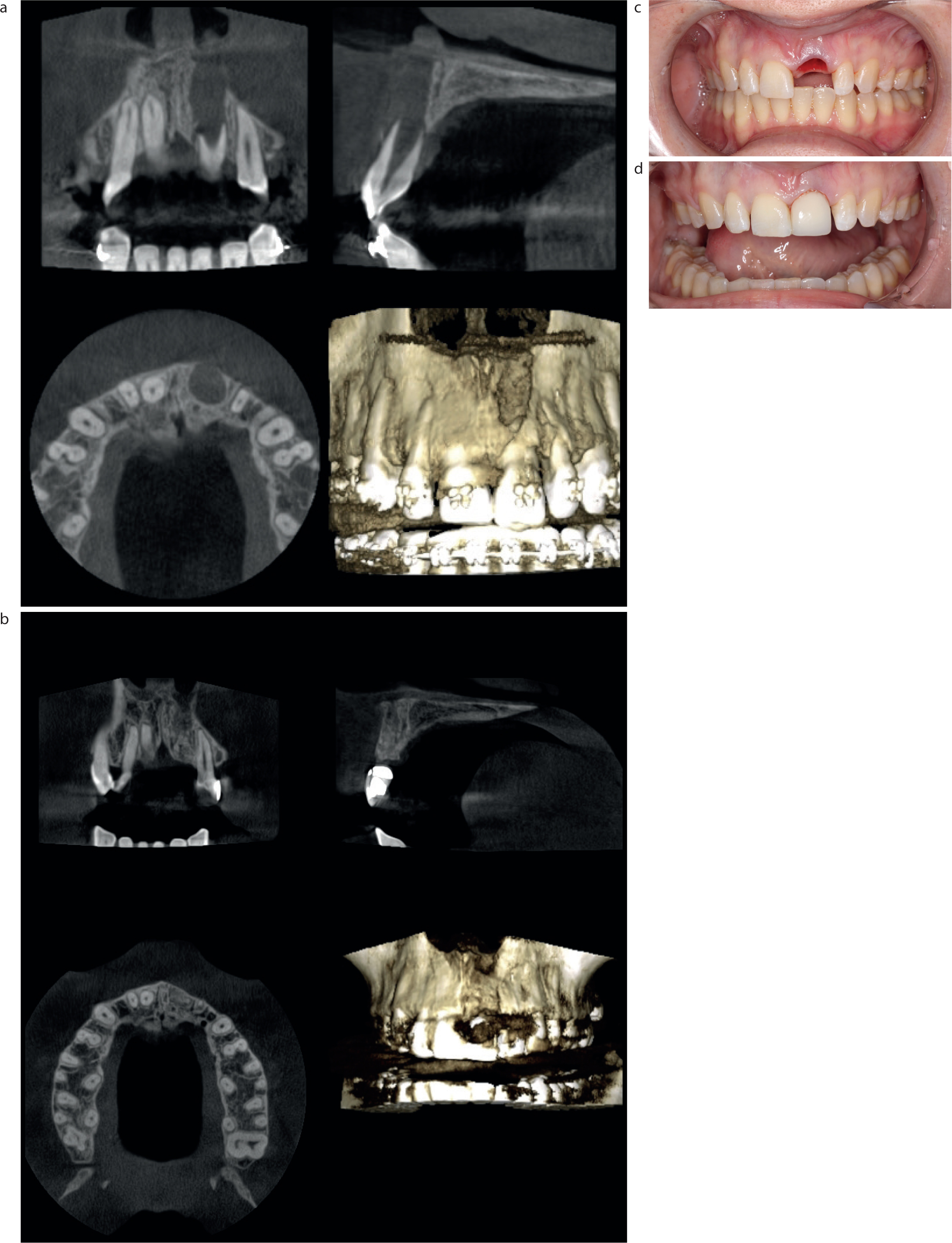
The case was reviewed following completion of orthodontic treatment and a cone beam CT (CBCT) scan taken (Figure 4a). This confirmed a significant apical defect with almost no residual bone for Type 1 or Type 2 implant placement. The case was further discussed at an MDT meeting, and it was agreed to carry out a ridge preservation treatment3,4 to help retain the hard and soft tissue contour, while also regenerating the apical defect (Figure 4b).
Figure 4. CBCT assessment of bone levels. (a) Before and (b) and after ridge preservation. (c) Extraction of UL1 (d) and fitting of temporary Maryland bridge.
In summary, the UL1 was removed atraumatically, and the apical tissue curretaged to bone (Figure 4c). Allograft bone substitute (Maxgraft, Botiss, Germany) was placed into the socket and a porcine collagen membrane sutured over the socket to close. A socket-fitted temporary Maryland bridge was then fitted as a temporary restorative measure (Figure 4d). The pontic was fitted into the socket to support the surrounding tissue and protect the graft.
Lateral incisor reshaping
As part of the overall treatment plan, the patient requested an improvement in the shape of both lateral incisors. This was carried out following a diagnostic wax-up using direct composite additions (Venus, Hereaus Kulzer, Kulzer Ltd, UK) (Figure 5).
Figure 5. Lateral incisor reshaping.
Implant surgery
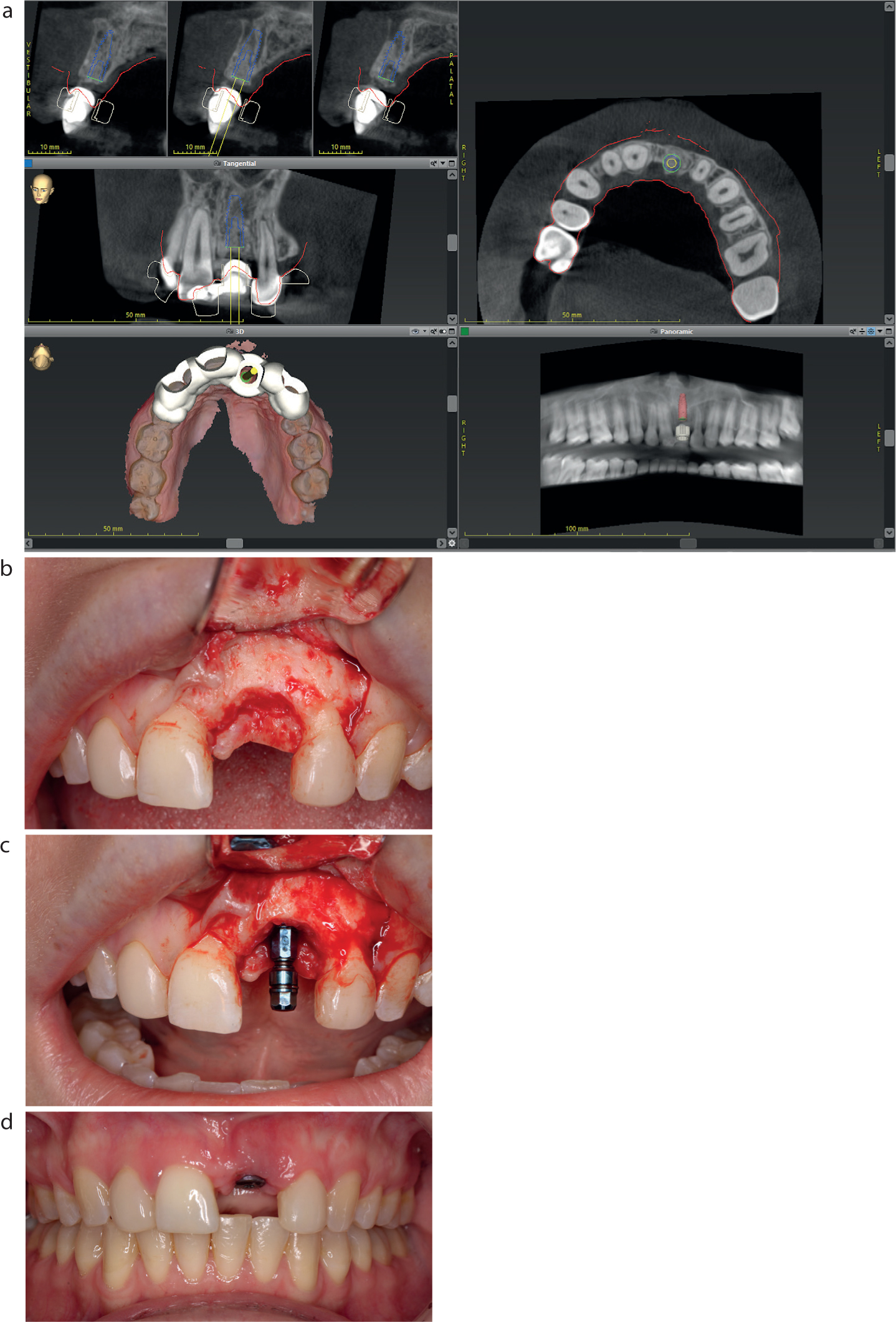
The ridge preservation was left to mature for 6 months before considering implant placement. CBCT showed good healing of the graft within the defect. Digital planning was then carried out using implant planning software (Co-Diagnostix, Dental Wings, Dental Wings GmbH, Germany) and a surgical guide was designed to enable accurate placement of the implant to achieve the optimal aesthetic result, as well as screw retention of the final crown (Figure 6).
Figure 6.
(a) Implant planning; (b,c) surgery; and (d) and fitting of healing abutment after 8 weeks of integration.
Implant placement was straightforward and uneventful as a result of the previous ridge preservation (Figure 6). A two-sided full-thickness mucoperiosteal flap was raised, and a surgical guide was used to prepare the pilot hole. The osteotomy was finalized, and a Straumann BLT 4.1 x 12 mm SLActive implant (Straumann, Switzerland) was placed. As there was in excess of 2 mm of bone buccal to the implant, no further augmentation was necessary at this stage. A cover screw was placed into the implant and primary closure was achieved using 5-0 Prolene (Ethicon, Johnson & Johnson Medical NV, Belgium).
The implant was then left to integrate for 8 weeks, and the Maryland bridge was refitted as a temporary restoration. After 8 weeks, the implant was exposed through a small crestal incision and a transmucosal healing abutment was fitted (Figure 6).
Implant reconstruction
As this tooth was in the aesthetic zone, a temporary implant restoration was fabricated to develop the soft tissue profile (Figure 7).5,6 Intra-oral scans were taken with a 3Shape Trios Scanner (3Shape, Denmark) and passed to the laboratory. A PMMA screw-retained crown was fabricated and then fitted.
Figure 7.
(a) Fitting of a temporary implant restoration allowed time for soft tissue profile to develop. (b) A final scan and shade match were taken.
Over the following 3 months, the crown was adjusted around the cervical margin to improve the shape and to help support the developing papillae. A final two-stage scan was then taken to capture the soft tissue profile. Shade-match photos were taken with a Vita Shade Guide (VITA Zahnfabrik, Germany) and passed to the laboratory (Figure 7), where a screw-retained zirconia crown supported by a custom titanium abutment was constructed.
The final crown fit appointment involved removal of the temporary restoration and fitting of the final crown. The crown was torqued to 35 Ncm and the screw channel sealed with PTFE and composite. The occlusion was checked to ensure that shimstock could pass through the crown and opposing tooth with light contact in ICP, and then during holding when the patient clenched together. This took the lack of periodontal ligament around the implant into account.
Post-operative photographs show a good shade match, with excellent soft tissue integration (Figure 8) and the patient was delighted with the final result.
Figure 8.
(a,b) Fitting of the final crown.
Conclusion
This case highlights the critical role of a dental multidisciplinary team in managing complex cases, such as the replacement of a failing maxillary central incisor. By integrating orthodontic, surgical and restorative disciplines, the team was able to achieve an outcome that satisfied both functional and aesthetic objectives.
The orthodontic space creation and alignment set the foundation for the restorative phase, ensuring that the UL1 could be replaced in an optimal position. Ridge preservation, guided by oral surgical principles, preserved hard and soft tissue contours, ensuring a solid foundation for implant placement. Finally, the restorative phase capitalized on these efforts, delivering a natural-looking prosthesis with excellent soft tissue integration.
Collaboration within the MDT facilitated seamless transitions between treatment phases, minimized risks, and ensured clear communication of patient expectations and goals. This case underscores that a coordinated multidisciplinary approach is paramount in achieving success in the most challenging dental scenarios. The patient's satisfaction with the outcome further emphasizes the value of integrating specialized expertise to deliver comprehensive care tailored to individual needs.
The MDT approach not only restored the patient's smile, but also contributed to long-term stability, functionality and confidence. This case demonstrates how such collaboration and communication is indispensable for achieving superior outcomes in complex dental treatments.