Andreasen JO, Sundström B, Ravn JJ. The effect of traumatic injuries to primary teeth on their permanent successors. I. A clinical and histologic study of 117 injured permanent teeth. Scand J Dent Res. 1971; 79:219-283 https://doi.org/10.1111/j.1600-0722.1971.tb02013.x
Torres CRG, Borges AB, Torres LMS, Gomes IS, Simões de Oliveira R. Effect of caries infiltration technique and fluoride therapy on the colour masking of white spot lesions. J Dent. 2011; 39:202-207 https://doi.org/10.1016/j.jdent.2010.12.004
Kim S, Kim EY, Jeong TS, Kim JW. The evaluation of resin infiltration for masking labial enamel white spot lesions. Int J Paediatr Dent. 2011; 21:(4)241-248 https://doi.org/10.1111/j.1365-263x.2011.01126.x
Paris S, Meyer-Lueckel H, Cölfen H, Kielbassa AM. Penetration coefficients of commercially available and experimental composites intended to infiltrate enamel carious lesions. Dent Mater. 2007; 23:(11)742-748 https://doi.org/10.1016/j.dental.2006.06.029
Cheng YL, Musonda J, Cheng H Effect of surface removal following bleaching on the bond strength of enamel. BMC Oral Health. 2019; 50 https://doi.org/10.1186/s12903-019-0742-4
Strnad G, Kovacs M, Andras E, Beresescu L. Effect of curing, finishing and polishing techniques on microhardness of composite restorative materials. Proc Technol. 2015; 19:233-238 https://doi.org/10.1016/j.protcy.2015.02.034
Lopes IAD, Monteiro PJVC, Mendes JJB, Gonçalves JMR, Caldeira FJF. The effect of different finishing and polishing techniques on surface roughness and gloss of two nanocomposites. Saudi Dent J. 2018; 30:197-207 https://doi.org/10.1016/j.sdentj.2018.04.003
An 18-year-old male patient presented with generalised hypoplasia affecting the appearance of his maxillary anterior teeth. Aiming to keep any restorative intervention as minimally invasive as possible, a combination of tooth whitening, particle abrasion, resin infiltration and direct composite masking were used in this case to deliver significant aesthetic improvement.
CPD/Clinical Relevance: This article explores minimally invasive approaches to restorative dental procedures and provides an understanding of the motivations for these approaches, the considerations for treatment planning and the impacts on treatment outcomes for patients.
Article
Minimally invasive dentistry embraces most aspects of patient care and supports a systematic respect for natural tissues. It includes prevention, diagnosis and minimal removal of hard tissues when restorative procedures are indicated.1 Advances in dental materials and adhesive technology also allow the principles of minimally invasive dentistry to encompass aesthetic dental treatments that are designed to enhance patient's self-confidence. Such procedures carry significantly lower biological and financial costs compared to indirect restorative procedures, as well as a reduced risk of complications, and are easier to repair or refurbish.1 A central tenet of the consent process is to present patients with all management options (including no treatment) along with relative risks, benefits and associated costs. This allows the patient's best interests and maintenance of oral health to be the primary focus of any treatment plan. This article describes the management of a patient with hypoplastic maxillary anterior teeth using minimally invasive tooth whitening, resin infiltration and direct adhesive restorative techniques.
Management of enamel hypoplasia with resin infiltration
Developmental enamel hypoplasia and traumatic dental injuries can manifest as white, yellow, or even brown discolourations on teeth. Hypoplasia is characterised by reduced enamel thickness, pits, opacities, and other irregularities.2 Although the hardness remains intact, there is a considerable variation in severity with regard to lesion extent and depth.2
Tooth whitening is the simplest and most minimally invasive method of treating brown and yellow discolourations. It may also be used in the management of white discolourations by reducing the contrast between opaque white spots/lesions and the background enamel colour. However, deep opaque white lesions can be more difficult to treat successfully with tooth whitening alone.
Enamel is the most highly mineralised tissue in the body and is made up of approximately 96% mineral and 4% organic material. In white lesions, the enamel is less mineralised and less organised, with organic fluids replacing part of the mineral phase. This results in differences in light refraction between lesions and healthy adjacent enamel, for example the refractive index of air is 1.0 compared to water, which is 1.33 and 1.0. Light changes course numerous times when entering white lesions altering the optical properties so that they appear brighter than the adjacent healthy enamel.
Resin infiltration was initially introduced as a method of stabilising incipient smooth surface carious lesions, but has now been widely indicated as a minimally invasive method for improving the aesthetic properties of teeth with opaque white lesions of varying aetiologies.3,5,5
Use of Icon resin infiltration (DMG, Hamburg, Germany) alters the refractive index of opaque white spots to 1.62, so that they appear similar to the refractive index of enamel, which is 1.65. This method avoids the need to physically remove the white spot lesion. It involves accessing the surface of the white lesion and using a low-viscosity resin that infiltrates the lesion driven by capillary forces.6 This process subsequently blends the refractive index of the white spot with the surrounding enamel, masking the lesions.2 The following clinical case report provides a step-by-step guide to the materials, equipment and clinical techniques used to treat a patient with severe enamel hypoplasia (Figure 1).
Figure 1.
Pre-operative appearance.
Clinical case
A healthy 18-year-old male patient seeking to improve his smile was referred via a university teaching hospital. He had previously been offered treatment plans involving direct or indirect veneers to address the appearance of his maxillary anterior teeth, which had hypoplastic defects affecting the aesthetic quality and quantity of enamel. The patient was classified as being at low risk of oral diseases and intra- and extra-oral examination revealed no positive diagnoses other than the following:
Localised gingivitis;
Significant developmental enamel hypoplasia, including pit/groove defects, missing enamel and a range of unaesthetic discolourations;
Shortened maxillary right lateral incisor.
Aesthetic assessment, diagnosis and treatment plan
The patient wished to ‘reduce the prominence of the white spots’ on his teeth. He had previously completed orthodontic treatment and had been offered between four and eight direct or indirect veneers. He had been informed that a layer of opaque material would be necessary to mask the white spot, potentially resulting in teeth with thicker and less natural proportions. The patient and his mother decided to seek a more minimally invasive solution to improve the appearance.
The patient consultation included discussion of the resin infiltration technique where the mineralised layer overlying the white spots is removed using hydrochloric acid, allowing a low viscosity resin to be infiltrated into the more porous, hypomineralised subsurface layers. As the resin has a refractive index close to that of healthy enamel, it allows the lesions to mimic the translucent properties of the unaffected adjacent tooth tissue.
The patient was also advised that the severity of his enamel hypoplasia was likely to necessitate the need for some localised enamel preparation. Particle air abrasion was recommended for the controlled, minimally invasive management of the unaesthetic defects followed by the use of a thin layer of direct composite to restore the natural contours of the labial surfaces.
With particular consideration given to the patient's young age, the patient and mother consented to the following minimally invasive treatment plan:
Supra- and sub-gingival professional mechanical plaque removal and prophylaxis;
Tooth whitening (to treat dark discolourations and reduce the need for masking);
Localised enamel preparation of white hypoplastic defects;
Resin infiltration of maxillary and mandibular labial surfaces;
Use of direct resin composite to restore labial surfaces to natural contour;
Direct restoration of the maxillary right lateral incisal edge to mirror the contralateral tooth.
Pre-operative treatment
Initial treatment consisted of preventive advice, professional mechanical plaque removal and review to ensure that a healthy periodontal condition had been established.
To treat the superficial yellow and brown discolourations, the patient then completed a 2-week course of home whitening, using 10% carbamide peroxide for 7 days followed by 16% carbamide peroxide for the subsequent week (LUMIWHITE, Yorkshire, UK). It was essential to maintain a minimum 7-day interval between the completion of tooth whitening and the restorative treatment to optimise bonding and to allow assessment of tooth colour stability.7
Pre-operative treatment included shade assessment using different samples of resin composite materials, which were polymerised (without etching) on a suitable labial surface. The material selected was Estelite Asteria (Tokuyama, Trycare, Bradford, UK) in shade WE (white enamel) (Figure 2).
Figure 2.
Shade selection using composite resin samples (light cured).
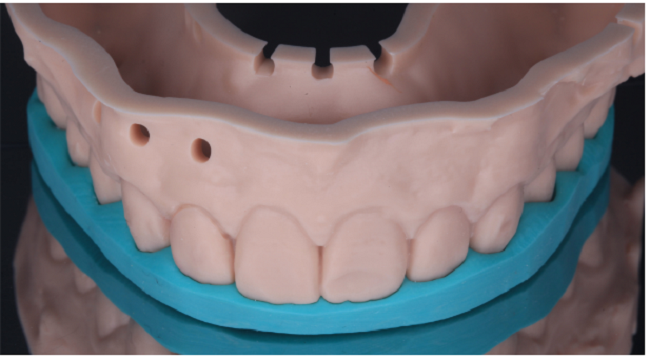
A digital wax-up was also made to design the incisal lengthening of the UR2, using UL2 as a guide. This also enabled construction of a palatal silicone template (Figure 3).
Figure 3.
Pre-operative silicone template made from a digital wax-up.
Resin infiltration techniques
The maxillary anterior teeth were isolated using rubber dam. The resin infiltration process began with localised application of 15% hydrochloric acid (Icon-etch, DMG) to the affected labial surfaces. This was left in place for 2 minutes and resulted in the removal of up to 50 µm of surface enamel (Figure 4).6
Figure 4.
Icon-etch (15% Hydrochloric acid) left for 20 seconds before thorough washing and drying.
The etch was rinsed with water for 30 seconds, and thoroughly dried to reveal the characteristic frosty etch pattern, before application of a 99% ethanol solution (Icon-dry, DMG). This is a critical step that enables assessment of whether the lesion will be adequately masked by resin infiltration. This etching and previewing process was repeated for 3–4 cycles. In this case, the depth of the hypoplastic lesions precluded complete masking. Therefore, following discussion with the patient, localised enamel preparation was carried out to assess and reduce the white lesions on the labial surfaces of the maxillary central incisors, sometimes known as ‘un-roofing’ of the lesion, or macro-abrasion.
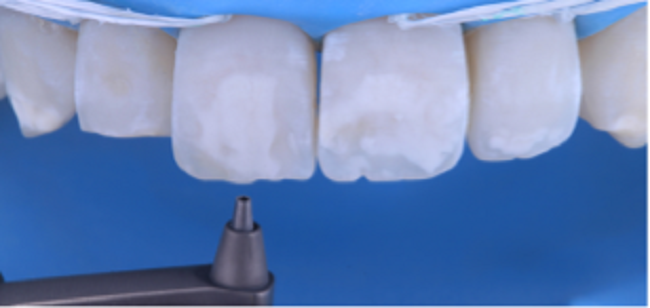
Tooth preparation was carried out using particle air abrasion with 27-µm aluminium oxide, for 30 seconds at a pressure of 2 bar (Figure 5) (Prepstart, Danville, USA).
Figure 5.
Particle air abrasion (27μm aluminium oxide).
The Icon-etch and Icon-dry were then repeated for two more cycles, augmented by further localised particle air abrasion.
Once the Icon-dry demonstrated satisfactory masking of the white spot lesions, the resin infiltration stage commenced.
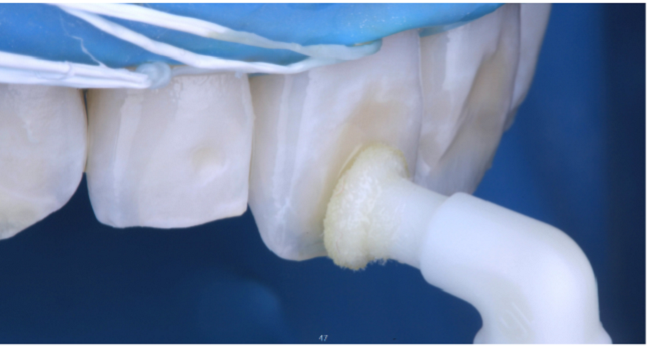
Icon resin was applied using a specialised applicator and agitated over a 2-minute period, before being left undisturbed for 1 minute to maximise penetration (Figure 6). Excess resin was removed by blotting with a dry microbrush and flossing interdentally. The resin was then light cured for 30 seconds at maximum power, and with the light tip as close as possible. A second layer of resin was then applied and light cured using the same protocol, before restoration of labial cavities with composite resin.
Figure 6.
Resin infiltration (Icon, DMG).
Direct composite restorations
Since the mid-1990s, composite resin materials have been successfully used to replicate the complex optical properties of translucent enamel and opaque dentine with a wide range of colourations.7 While incremental layers of composite resin can be used to achieve natural-looking restorations, the use of resin infiltration can reduce the need for advanced layering techniques. This changes the primary function of the composite from masking any remaining white spots, to creating a smooth, homogeneous restorative surface. In many cases, the selected composite can be achromatic, allowing the natural tooth colour to show through the resin material.
In this case, the composite material of choice was Estelite Asteria (Tokuyama, Trycare, Bradford, UK) This is a highly filled (82% by weight), nano-hybrid material with excellent handling properties and polishability. The material is available in seven opaque dentine shades (Body shades: A1B, A2B, A3B, A3.5, A4B, B3B and BL) and five enamel shades: NE (natural enamel), WE (white enamel), YE (yellow enamel), TE (trans enamel) and OcE (occlusal enamel). In this case, a single shade of WE (white enamel) was suitable for the majority of the restorative procedure.
For the incisal restoration of the maxillary right lateral incisor, the pre-operative silicone palatal template (Figure 7), made from the digital wax-up, was used for the controlled integration of function and aesthetics, using the following material sequence:
Each increment was light cured for 30 seconds, with a final 60-second light cure under a barrier medium (Liquid Strip, Ivoclar Vivadent, Liechtenstein) to eliminate the oxygen inhibition layer and optimise surface hardness and stability.8
In this case, the restorations were initially shaped at the first appointment, but not fully polished. The patient returned 1 week later for completion of a full polishing protocol that comprised a range of composite finishing discs, which have been demonstrated to produce optimal surface smoothness and gloss using scanning electron microscopy:9
Stage 1 (Sof-Lex discs, 3M ESPE);
Stage 2 (Astropol, Ivoclar Vivadent).
Treatment outcome
In this case, the minimally invasive approach resulted in a successful outcome that greatly improved the patient's aesthetic appearance (Figures 8 and 9). The conservative nature of the treatment maximised preservation of the patient's natural tooth structure and reduced the risk of complications.
Figure 8.
(a) Pre-operative and (b) post-operative close-ups (with contraster).
Figure 9.
(a) Pre-operative and (b) post-operative portraits.
At all stages of treatment, care was taken to effectively manage expectations, resulting in a high level of patient satisfaction with the improvement to his smile.
The long-term success of the treatment will ultimately depend on the patient continuing to optimise home care and attending for regular review appointments and restorative maintenance when necessary. However, it must be made clear that there is no long-term evidence in shade stability on resin-infiltrated teeth. This being said, if further whitening is to be sought, as this will eventually relapse, then palatal spacers will need to be used to ensure effective peroxide penetration into the tooth.
The case was rewarding for the patient and clinician alike, and demonstrated the benefits of optimising the materials, equipment and minimally invasive techniques incorporating resin infiltration.