Banerji S, Sethi A, Dunne SM, Millar BJ Clinical performance of Rochette bridges used as immediate provisional restorations for single unit implants in general practice. Br Dent J. 2005; 199:771-775 https://doi.org/10.1038/sj.bdj.4813027
Suarez-Feito JM, Sicilia A, Angulo J Clinical performance of provisional screw-retained metal-free acrylic restorations in an immediate loading implant protocol: a 242 consecutive patients' report. Clin Oral Implants Res. 2010; 21:1360-1369 https://doi.org/10.1111/j.1600-0501.2010.01956.x
Ray-Chaudhuri A, Ray-Chaudhuri E, Banki F Technique tips: temporary adhesive bridges. Dent Update. 2020; 47:612-613
Hussey DL, Pagni C, Linden GJ Performance of 400 adhesive bridges fitted in a restorative dentistry department. J Dent. 1991; 19:221-225 https://doi.org/10.1016/0300-5712(91)90122-f
Edelhoff D, Liebermann A, Schubert O, Güth JF Prospective clinical split-mouth study of two-wing–retained resin-bonded anterior fixed dental prostheses with metallic and ceramic frameworks: 5-year results. Int J Prosthodont. 2023; 36:253-261 https://doi.org/10.11607/ijp.7765
Bereznicki T, Dawood A The creation of an emergence profile, part I. Using an interim restoration as an aid to implant positioning. Dent Today. 2012; 31:126-129
Bereznicki T, Dawood A The creation of an emergence profile, part 2: pontic-guided implant placement in the aesthetic zone. Dent Today. 2012; 31:68-71
Use of an immediate adhesive temporary bridge to create an emergence profile Tom Bereznicki Aesthetic Update 2025 2:1, 49-52.
Authors
TomBereznicki
BDS(Edin), FDSRCSEd(ad hom), MFDTEd, FCGDent, MFDSEng, Partner Associate Lecturer delivering the new PG Diploma in Advanced Aesthetic and Restorative Dentistry at the University of Portsmouth; Member of theTeaching Faculty of Kings College Dentistry Aesthetic Masterclass MSc Course
A description of the use of an immediate adhesive bridge to create a desired emergence profile prior to implant placement.
CPD/Clinical Relevance: To describe a method for establishing an optimal emergence profile.
Article
The case presented exemplifies a clinical approach wherein a fixed provisional restoration is provided to the patient in advance of implant placement. This provisional restoration is designed to be periodically removable, facilitating iterative adjustments to the pontic morphology. Such modifications are pivotal in establishing an optimal emergence profile. Consequently, this approach enables precise implant positioning, contingent upon sufficient bone width, thereby enhancing the final aesthetic outcome (Figures 1–9).
Figure 1.
(a–c) These pictures illustrate a clinical scenario involving four failing maxillary anterior teeth. The patient strongly declined the use of a removable immediate partial denture, explicitly opting instead for an adhesive bridge. Given the patient's elevated lip line, achieving optimal gingival aesthetics significantly influenced this treatment decision. The use of a meticulously designed adhesive bridge, permitting periodic removal during the 3-month post-extraction healing interval, enables incremental modifications to its surface. Such adjustments facilitate directed tissue healing and sculpting, ultimately promoting the formation of an ideal ovate pontic architecture for subsequent definitive implant-supported restoration.Figure 2.
(a,b) An illustration of an adhesive bridge demonstrating metal retentive wings extended onto the buccal surfaces of the abutment teeth to enhance stability whenever aesthetically feasible. Since this bridge serves as a provisional restoration placed without enamel preparation, the additional buccal support significantly contributes to retention and stability. In cases where limited palatal surface area on the abutment teeth is available for adhesive bonding, the incorporation of retention perforations, analogous to those used in the original Rochette bridge design, can further improve retention, as exemplified in (b). Composite resin or acrylic materials are recommended for pontic fabrication, as their inherent properties allow for efficient and straightforward incremental modifications when clinically indicated.Figure 3.
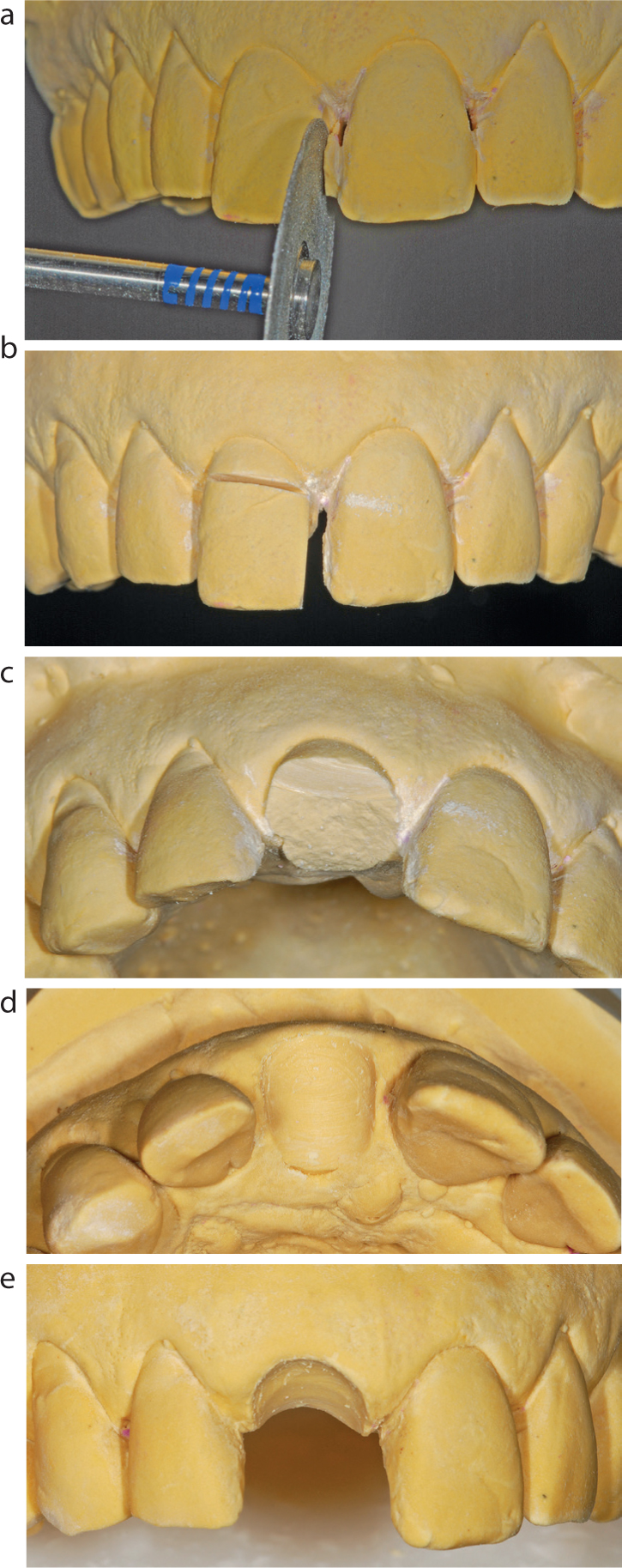
(a–e) Demonstration of the critical aspect underpinning the success of this technique, specifically emphasizing that the pontic must be meticulously designed with a socket-fitted form rather than adopting a ridge-lap configuration. The procedural steps involved in trimming the working model to achieve an accurate and anatomically congruent socket-fit pontic are succinctly illustrated.Figure 4.
(a,b) Distinct illustration of the extraction site, explicitly revealing the socket morphology into which the pontics must achieve a passive and precise fit. Provided the working models have been accurately contoured, the adhesive bridge is expected to seamlessly seat into position, eliminating the necessity for additional chairside adjustments.Figure 5.
(a–c) Illustration of the adhesive bridge at the point of clinical placement, clearly demonstrating the extended retentive elements positioned on the buccal surfaces to enhance stability. This provisional adhesive bridge is fitted immediately following tooth extraction. Moisture control during cementation can be effectively managed either by employing a modified dental dam technique or through continuous suction. Considering the provisional nature of this restoration and the requirement for ease of removal, the standard of moisture control during cementation is less rigorous than that typically necessary for a definitive adhesive bridge.Figures 6.
(a–c) Illustration of clearly visible alveolar ridge resorption at the fifth week post-extraction. Caution is advised when selecting the cementation medium. Using an adhesive resin cement, such as Panavia (Kuraray, Japan) may result in fracturing of the palatal enamel shelf upon application of force during bridge removal. Alternatively, the use of a resin-modified glass ionomer cement (RMGIC) is recommended because this preserves enamel integrity. GC Fuji Triage Pink (GC, Japan), a specific type of RMGIC, offers the added advantage of easy identification and removal during maintenance appointments. Upon removal of the provisional restoration, incremental additions to the pontic areas can be carried out approximately every 3 weeks. This process is instrumental in guiding soft tissue healing and specifically encouraging papilla formation throughout the 3-month period of alveolar bone healing.Figure 7.
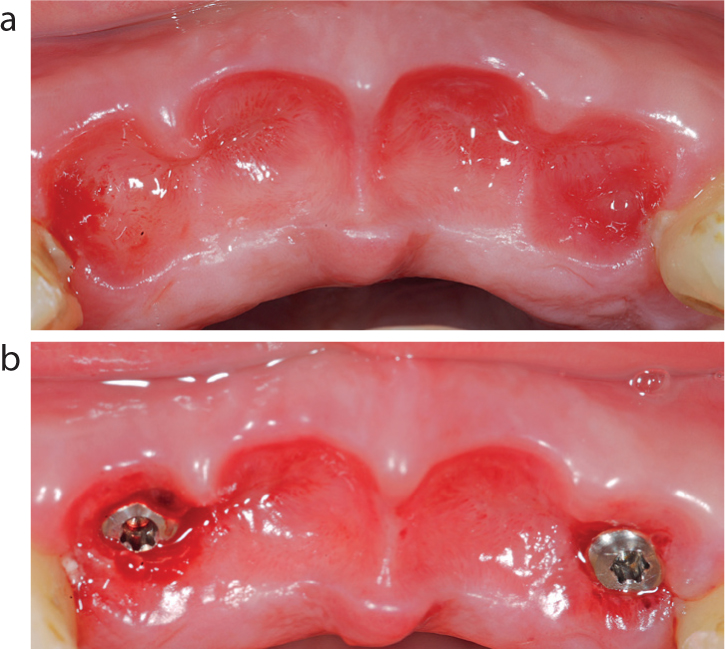
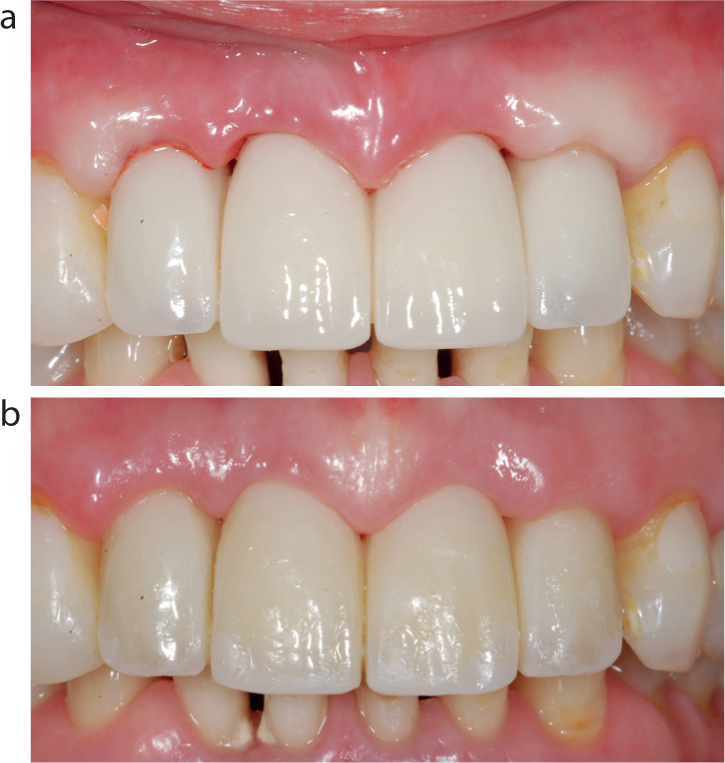
(a,b) Illustration of the emergence profile achieved following approximately 3 months of guided soft-tissue management. At this stage, implant placement can proceed, as demonstrated in (b). Provided there is adequate bone volume, both in height and width, implants can be accurately positioned to facilitate optimal aesthetic outcomes for the definitive implant-supported bridge.Figure 8. On implant placement, the provisional adhesive bridge can be adapted around the implants, but a high level of oral hygiene can be difficult to maintain between the healing abutments and the adapted pontics. The preferred protocol is to provide, where occlusal conditions permit, a screw-retained immediate-load bridge on the same day as implant placement. The clinical appearance (a) immediately after fitting the bridge and (b) 20 days post-placement. Notably, rapid soft tissue adaptation and papillary formation around the immediate-load restoration can be clearly observed.Figure 9.
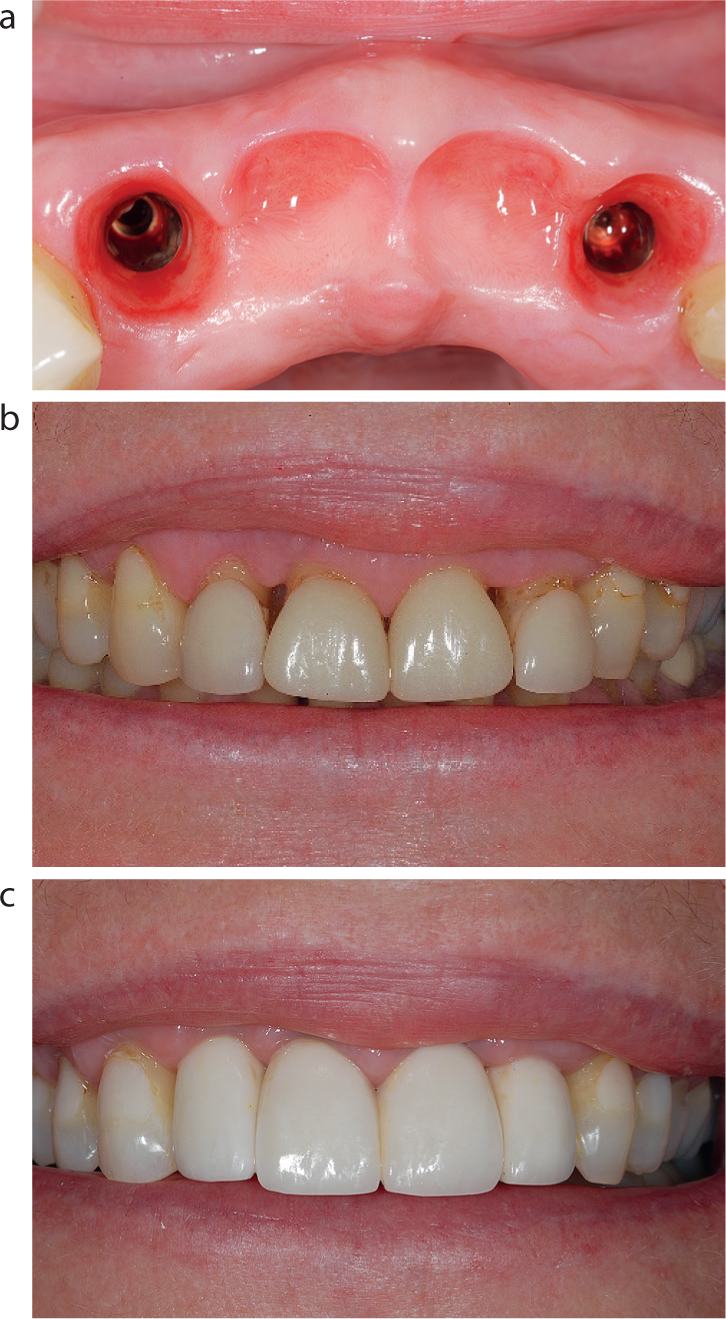
(a) Illustration of the soft tissue presentation observed upon removal of the immediate-load bridge, 3 months following implant placement and osseo-integration. It is imperative that this immediate-load restoration remains undisturbed throughout the entire 3-month integration period. Clinicians should note that the soft tissue profile tends to collapse rapidly upon bridge removal.6,7 Thus, an appropriate duplication technique needs to be applied to mitigate potential inaccuracies in capturing the established emergence profile. (b) The clinical situation prior to the commencement of the treatment. (c) The completed post-treatment aesthetic outcome depicting the soft tissue contours and the high lip line. The definitive bridge demonstrates excellent aesthetic integration, clearly evidenced in (c), although the selected shade reflects the patient's own preference.
Considerations regarding material selection
The selection of the original non-precious metal framework remains preferential in clinical practice, primarily attributable to its advantageous mechanical properties. Specifically, this material provides exceptional structural robustness, particularly beneficial in preserving integrity within thin retentive wing sections. Additionally, the non-precious metal framework affords superior marginal adaptation and has consistently demonstrated favourable long-term clinical outcomes. To further augment the stability of adhesive bridges and minimize the potential for unintended debonding, it is advised, where anatomically and aesthetically feasible, to extend the retentive wings onto the buccal surface. This design modification significantly enhances mechanical retention and structural stability. Moreover, in clinical situations characterized by restricted palatal surface availability on the abutment teeth, introducing retention perforations similar to those employed in the original Rochette bridge design is advisable.1 This method, supported by extensive clinical evidence, has been shown to substantially increase retention efficacy. Importantly, this approach demonstrates considerable durability and longevity.2,3,4,5 Considering the necessity for periodic removal and re-insertion of the prosthesis during treatment progression, the risk of framework fracture remains notably low, underscoring the reliability of this material choice.
Considerations for the pontic material
The use of porcelain as a pontic material is generally contraindicated within this clinical protocol owing to inherent limitations in achieving dependable adhesion and predictable incremental modifications to the pontic morphology. Consequently, clinicians should preferentially select composite resin or acrylic-based materials, which are advantageous in permitting straightforward and predictable chairside modifications. The inherent flexibility of these materials facilitates efficient and accurate alterations to the pontic shape, thus enhancing clinical outcomes and patient satisfaction.
Reflections on zirconia as a framework material
Although zirconia has been increasingly explored as a potential framework material in dental prosthetics, its application within the current adhesive bridge protocol presents substantial clinical limitations. Notably, zirconia frameworks incorporating thin retentive wings carry a significantly elevated risk of fracture under functional loads, particularly during repeated prosthesis removal procedures. Additionally, the intrinsic brittleness of zirconia precludes buccal extensions designed to improve stability, because such modifications would inherently compromise structural integrity. Furthermore, retention perforations, useful in metal frameworks to improve cementation when surface area is insufficient, are contraindicated for zirconia, as their presence would critically weaken the retainers and predispose them to structural failure.
Moreover, zirconia pontics present distinct limitations concerning post-fabrication adjustments. The technical complexity and clinical unpredictability associated with adhering composite resin or acrylic materials to zirconia surfaces further diminish its practicality. Indeed, attempts to add composite or acrylic onto zirconia surfaces frequently result in rapid delamination, thereby undermining prosthesis longevity and clinical reliability.